Download
1 / 43
450 likes | 676 Views
The Role of Glucokinase in Non-Insulin-Dependent (Type 2) Diabetes. Presenter: Beth Prentice.

E N D
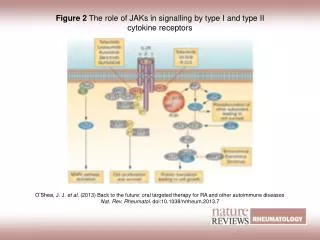
The Role of Glucokinase in Non-Insulin-Dependent (Type 2) Diabetes Presenter: Beth Prentice Slosberg E, Desai U, Fanelli B, St. Denny B, Connelly S, Kaleko M, Boettcher B, Caplan S. 2001. Treatment of type 2 diabetes by adenoviral-mediated overexpression of the glucokinase regulatory protein. Diabetes 50:1813-20.
Presentation Outline INTRODUCTION Types of Diabetes Understanding Type 2 Diabetes Symptoms and Complications Treatment for Type 2 Diabetes Patient Self-Care PRIMARY ARTICLE - RESEARCH/DATA What is glucokinase (GK)? GKRP? Treatment of Type 2 Diabetes by Adenoviral-Mediated Overexpression of the Glucokinase Regulating Proteins CONCLUSION Summary
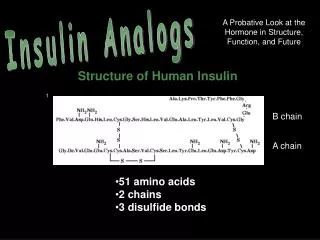
Two primary types of diabetes affecting 16 million people in the United States Type 2 diabetes (non-insulin-dependent diabetes mellitus) accounts for of those affected Type 1 diabetes (insulin-dependent diabetes mellitus) accounts for of those affected 10% 90%
Type 1 diabetes: insulin production stops Insulin helps glucose (sugar) move into cells, where it is used to produce energy Without insulin, glucose cannot enter the cells Cells quickly waste away from lack of glucose INSULIN INSULIN CELL INSULIN CELL CELL
Type 2 diabetes: insulin production and effectiveness are impaired Insulin helps glucose move into cells, where it is used to produce energy If not enough insulin is produced (insulin deficiency), not enough glucose can move into cells When insulin is not used properly (insulin resistance), cells do not respond by taking in glucose Cells slowly waste away from lack of glucose INSULIN INSULIN CELL INSULIN INSULIN CELL INSULIN CELL
Normally, the body regulates blood glucose levels by removing excess glucose after a meal... Ingested carbohydrates are metabolized into glucose and absorbed into the blood, causing high blood sugar (hyperglycemia) The pancreas produces and secretes insulin, which helps move glucose into cells Blood glucose levels return to normal Muscle, fat, and liver cells take up glucose from the blood
…and releasing stored glucose back into the blood between meals Gastrointestinal tract is empty; glucose must be supplied by the body for energy The pancreas produces and secretes glucagon, stimulating the liver to release the glucose stored during meals The liver releases glucose in response to low blood sugar (hypoglycemia) Blood glucose levels return to normal
Normally, the body keeps glucose levels from rising too high... Carbohydrates, metabolized into glucose, are absorbed into the blood Too High Normal Too Low Blood glucose increases to higher than normal levels (hypergly-cemia) The pancreas secretes insulin, helping uptake of glucose by muscle, fat, and liver cells Glucose moves quickly out of the blood into the cells
…and falling too low Too High Normal Too Low Gastrointestinal tract is empty; glucose must be supplied by the body Blood glucose decreases to lower than normal levels (hypogly-cemia) The pancreas secretes glucagon, stimulating the liver to release glucose Glucose is released from the liver into the blood
Type 2 diabetes evolves from 2 primary defects: insulin deficiency and insulin resistance Progression of untreated type 2 diabetes Glucose is absorbed into the blood, causing hyperglycemia Pancreatic dysfunction leads to insulin deficiency Muscle, liver, and fat cells develop insulin resistance Blood glucose levels remain high
With type 2 diabetes, glucose levels stay high for a longer time... Too High Normal Too Low Carbohydrates are metabolized into glucose and absorbed into the blood Muscle, fat, and liver cells are insulin resistant; glucose stays in the blood Due to an increase in blood glucose concentration, the liver produces glucose Because it moves slowly into the cells, glucose levels stay high for longer than normal
…and fall more slowly Too High Normal Too Low Hyperinsulinemia results from a release of too much insulin in response to glucose levels that remain high from the previous meal Movement of glucose out of the blood into cells eventually outpaces the release of glucose from the liver Gastro-intestinal tract is empty; glucose is supplied by the liver Glucose levels do not return to normal
Early symptoms are unpleasant... Excessive eating (polyphagia) and drinking (polydipsia) Excessive urination (polyuria) Dramatic weight changes (sudden loss or excessive gain) Genital itching and infections in women; impotence in men
…and can be significant Blurred vision Weakness, tiredness, or dizziness; inability to concentrate; loss of coordination; loss of consciousness Slow-healing cuts or sores; frequent skin and urinary tract infections Nausea and vomiting Numbness or tingling in hands or feet
Eye disease (retinopathy) Nerve damage (neuropathy) Gum disease Skin disorders Later complications can be quite serious...
…and can often be life threatening Myocardial infarction, congestive heart failure, hypertension Peripheral vascular disease, stroke Kidney disease (nephropathy) Gangrene and amputations
Patients’ nutrition therapy is an essential part of total diabetes care Restrict caloric intake (by 250 to 500 calories per day) Limit salt intake (<3000 mg sodium per day) Limit fat intake (total fat <30% of total calories; saturated fat <10% of total calories)
Increased physical activity is vital to diabetes management Physical activity (such as walking) may improve insulin sensitivity Physical activity can lower blood glucose to normal levels
Drug therapy is needed in addition when diet and physical activity fail to correct hyperglycemia Insulin for type 1 or type 2 diabetes Oral hypoglycemic agents for type 2 diabetes
Treatment of Type 2 Diabetes by Adenoviral-Mediated Overexpression of the Glucokinase Regulating Proteins
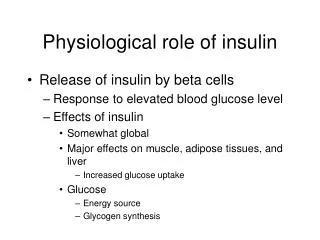
What is Glucokinase? • Glucokinase is produced in the liver. • It is an important component in maintaining glucose homeostasis in the entire body. • Glucokinase does this by catalyzing the phosphorylation of glucose in cells that express this enzyme. pancreatic β cells
The Role of Glucokinase • Glucokinase is critical in maintaining normal blood glucose and insulin levels. • Non-insulin-dependent patients have a reported decrease in glucokinase enzymatic activity. • Slight alterations in glucokinase protein levels has a great effect on maintaining normal blood glucose levels.
What is GKRP? • Glucokinase Regulatory Protein • In the liver, glucokinase activity is regulated by binding to the glucokinase regulatory protein (GKRP). • Function: GKRP inhibits GK activity under low-glucose conditions • GKRP has been identified in the regulation of glucokinase, and has been postulated as a candidate gene for type-2 diabetes.
Treatment of Type 2 Diabetes by Adenoviral-Mediated Overexpression of the Glucokinase Regulating Proteins
Objective of Study • Slosberg, et al. were interested in looking at the effect of increasing the hepatic levels of glucokinase regulatory protein (GKRP) on the diabetic phenotype of mice maintained on a high-fat diet.
The Effect of GKRP Over-Expression on the Rate of Glucose Phosphorylation
Fasting Blood Glucose Values in Vector-Treated Mice HBSS Null 300 GKRP LF: HBSS 250 200 Fasting blood sugar glucose (mg/dl) 150 100 50 0 Pre-inject 1 week 2 weeks 3 weeks
Null mice had lower fasting blood sugar levels than HBSS mice at all times tested. HBSS Null 300 GKRP LF: HBSS 250 200 Fasting blood sugar glucose (mg/dl) 150 100 50 0 Pre-inject 1 week 2 weeks 3 weeks
GKRP mice showed significant decrease in fasting glucose levels compared with both null and HBSS mice at all times tested. HBSS Null 300 GKRP LF: HBSS 250 200 Fasting blood sugar glucose (mg/dl) 150 100 50 0 Pre-inject 1 week 2 weeks 3 weeks
At the end of the experiment GKRP mice were indistinguishable from non-diabetic LF-HBSS mice. HBSS Null 300 GKRP LF: HBSS 250 200 Fasting blood sugar glucose (mg/dl) 150 100 50 0 Pre-inject 1 week 2 weeks 3 weeks
The Effect of Av3hGKRP Treatment on GK Protein and Activity in vitro
The effect of Av3hGKRP treatment on GK protein and activity 60 50 40 GK Activity 30 20 10 0 Av3Null Av3hGKRP Av3hGKRP + Av3hGK Av3hGK
Western Blot Analysis GKRP GK