Download
1 / 28
650 likes | 1.09k Views
Role of Time In Range And <br>Recommendation In the Basal Insulin Strategy<br>

E N D
Role of Time In Range And Recommendation In the Basal Insulin Strategy Dr Shahjada Selim Associate Professor Department of Endocrinology & Metabolism Bangabandhu Sheikh Mujib Medical University Faculty in Endocrinology, Texila American University, USA Website: http://shahjadaselim.com
Poll #1 According to you which is the most clinically relevant reason that misreads glycemic control from A1C alone? • Does not take hypoglycemia into consideration • Does not reflect inter- & intra-day glycaemic excursions • Unreliable in conditions such as pregnancy, hemoglobinopathies, anaemia (widespread in emerging countries) • Ethnic & racial differences in glycation • B. Does not reflect inter- & intra-day glycaemic excursions
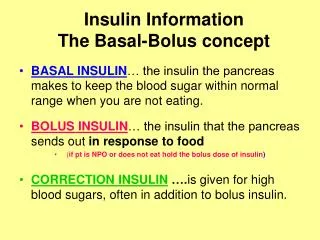
Why Do We Need a Monitoring Tool Beyond A1C? Inter and intraday glycemic excursions1 Recognize hypoglycemia1 HbA1c alone may not be sufficient Hemoglobinopathies, anemia & pregnancy1 Ethnic and racial differences2 Adjust the treatment regimen when the levels are elevated1 Personalized diabetes management1 HbA1c: Glycosylated hemoglobin. Danne T, et al. Diabetes Care. 2017;40:1631–1640.
From Triad to Hexad: Increasing Range of Targets in DM FPG-Fasting plasma glucose; PPG-Postprandial plasma glucose; GV- Glycemic Varibility; DM- Diabetes Mellitus Kalra S et.al. Pentads and hexads in diabetes care: Numbers as targets; Numbers as tools. Indian journal of endocrinology and metabolism. 2017 Nov;21(6):794.
Why Is Time-in–Range Important? Glycemic Variability? Patients at same A1C levels can have different TIR profiles Time-in–range can capture these differences in a way A1C cannot Patients experience different energy levels, moods, QoL when they are ‘in-range’ vs. ‘out-of–range.’ HbA1c:Glycated hemoglobin. Going Beyond A1c – One Outcome Can’t Do It All. Available at: https://diatribe.org/BeyondA1c. Accessed on: 31 January 2020.
‘Time-In-Range’ & What’s Above/ Below From ‘In-Range’? People with diabetes should spent Above target glucose range In a blood glucoserange of 70–180 mg/dL At least 17 hours a day, more than 70% of their time (3.9-10 mmol/L) Level 2 hyperglycemia Minimize (>13.1 mmol/L) Level 1 hyperglycemia (10-13.1 mmol/L) >17 hours Target in glucose range Time-In-Range Below target glucose range (3.9-10 mmol/L) (3.9-10 mmol/L) Level 1 hypoglycemia <1 hour (3.1-3.9 mmol/L) Level 2 hypoglycemia (<3.1 mmol/L) Battelino T, et al. Diabetes Care. 2019 Aug;42(8):1593-1603, Advani A. Diabetologia. 2020;63(2):242–252.
Poll #2 According to you which is the most valuable additional information furnished from TIR over A1C ? • Understand the current status & control of diabetes in real-time • Guide the requirement of change of therapy without delay • Useful for comparison of interventions • Understand improvement in hypoglycemia and hyperglycemia which otherwise cannot be ascertained D. Understand improvement in hypoglycemia and hyperglycemia which otherwise cannot be ascertained
ATTD 2019 Recommendations on TIR for Different Diabetes Populations % of readings; time per day: >70%; >16 h, 48 min Target range: 70–180 mg/dL (3.9–10.0 mmol/L) . Battelino T, et al. Diabetes Care. 2019;42(8):1593–1603. ATTD: Advances Technologies & Treatments for Diabetes CGM: Continuous glucose monitoring
Strong Association of TIR with Risk of Microvascular Complications in DCCT Trial TIR: Time in range; DCCT: Diabetes Control and Complications Trial Beck RW, et al. Diabetes Care. 2019;42(3):400-405.
Inverse Correlation of DPN with TIR . • Prevalence of DPN is inversely correlated with TIR • DPN prevalence was 43% and 74% among participants who were within the target range >70% and <70% of the time, respectively 74% 70% • For every 10% lower TIR there is a 25% increased risk of DPN • There was no significant association of HbA1c with DPN symptoms 43% Mayeda L, et al.BMJ Open Diab Res Care. 2020;8:e000991.
TIR and Carotid Intima-media Thickness Patients with abnormal CIMT showed significantly lower TIR values compared to patients with normal CIMT Prevalence of abnormal CIMT gradually decreased across the categories of increasing TIR TIR was significantly associated with CIMT in males but not in females TIR: Time-in-range; CIMT: Carotid intima media thickness Lu J, et al.Diabetes Technology & Therapeutics. 2020; 22(2):72-78.
Association of TIR with Outcomes Following Cardiac Surgery • Diabetic patients with TIR > 80% show better postoperative outcomes like decreased length of ICU stay & reduced incidence of wound infection Both diabetics and non-diabetics with low TIR (<80%) had poorer outcomes, as shown by length of stay and post-operative atrial fibrillation TIR: Time in range Omar AS, et al. BMC Anesthesiology. 2015;15(1):14.
Stay In Range To Avoid Unwanted Risks in Pregnancy Murphy HR. Diabetologia. 2019;62:1123-1128. TIR: Time in range; TAR: Time above range; LGA-Large for gestational age
In a Nutshell: What are the outcomes if TIR is not maintained? Retinopathy risk increases by 64% TIR lesser by 10% Nephropathy risk increases by 40% Neuropathy risk increases by 25% Initial evidences also show increase in the surrogate markers of macrovascular complications like abnormal carotid intima-media thickness2. Mayeda L, et al.BMJ Open Diab Res Care. 2020;8:e000991. Battelino T, et al. Diabetes Care. 2019;42(8):1593–1603. Beck RW, et al. Diabetes Care. 2019;42(3):400-405.
Poll #3 We have seen data that increase in TIR correlates to less CV complications. In absence of extensive evidence, from clinical experience does staying in range lead to CV benefits? Yes – Staying in range leads to CV benefits No – Staying in range does not lead to CV benefits A. Yes – Staying in range leads to CV benefits
Basal Insulin Strategies for • Time-In-Range: • How Gla-300 can Contribute?
18 Basal Insulin Can Effectively Address GV 1. Monnier L, Diabetes Care. 2002;25:737-741; 2. Mi-Kyung KIM. J Diabetes Metab. 2016;7:645; 3. Hanefeld M, et al. Diabet Med. 2010 Feb;27(2):175-80; 4. American Diabetes Association. Diabetes Care. 2018;41(Suppl 1):S73–S85; 5. Riddle MC, et al. Diabetes Care. 2003;26(11):3080-6; 6. Janka HU, et al. Diabetes Care. 2005;28:254–259. 7. Raskin P, et al. Diabetes Care. 2005;28(2):260–265.8. Kumar S, et al. Diabet Med. 2017;34(2): 180–188. 9. Kumar A, et al. PLoS ONE. 2016;11(10):e0163350.
Early Basal Insulin Initiation Is Suggested In These Challenging Times Basal insulin - the second-line after metformin in uncontrolled T2D 19 Hirsch IB. JAMA June 16, 2020 Volume 323, Number 23
Evolution Of Basal Insulin Development From 1st to 2nd Generation Basal Insulin Analogs: Overcoming Limitations Longer-acting basal insulins,insulin glargine 300 U/mL (Gla-300) andinsulin degludec (IDeg), have since been developed with less variability and more prolonged durations of action (>24 h)1,2 Insulin glargine 100 U/mL (Gla-100) andinsulin detemir (IDet) were developed to overcome some limitations of early basal insulins such as NPH insulin, with less variable absorption and longer duration of action1,2 IDet IDeg Gla-300 Gla-100 NPH Timeline 2010 2011 1996 1992 1946 Profile comparisons NPH, neutral protamine Hagedorn. IDet, insulin detemir. IDeg, insulin degludec1. Eliaschewitz FG, Barreto T. DiabetolMetabSyndr. 2016 Jan 6;8:2; 2. Adapted from Pettus J et al. Diabetes Metab Res Rev. 2016 Sep;32(6):478-96 20
Poll #4 According to you, which among the following is the most important factor in managing GV & TIR with insulin? Timely insulinization & choice of insulin Adequate initiation dose & proper titration Simple regimen with flexibility in dosing Prompt intensification with addition of bolus A. Timely Insulinization & choice of insulin
Improved GV With Gla-300 Irrespective Of Injection Timing Similar A1C reduction* with Gla-300 (-0.44%) vs Gla-100 (-0.22%) [p>0.05] • 24-h glucose curves Smoother profile with Gla-300 irrespective of morning or evening injection • Nocturnal hypoglycemia Lower for Gla-300 group than for Gla-100 group (4.0 vs. 9.0 events per participant-year; rate ratio 0.45 [95% CI 0.24–0.82]) * - not statistically significant (p>0.05) Bergenstal RM et.al. Diabetes Care 2017;40:554–560
Gla-300 Allows Flexibility in Injection Timings to Deal with Situational Variability in Day to Day Life 6-hour flexible dosing time window Pooled EDITION 1 and 2 substudies in T2DM (Months 6–9) Fixed dosing time Gla-300 may allow some flexibility in timing injections to deal with the situational variability experienced in daily life Flexible dosing time: - 3 hours Flexible dosing time: + 3 hours *Flexible dosing time: Once-daily injection intervals of 24 ± 3 hAdapted from Riddle M et al. Diabetes TechnolTher. 2016 Apr;18(4):252-7
Gla-300 Demonstrate Lower Nocturnal GV Compared To Ideg and First Gen. Basal % of time in nocturnal hypoglycemia with Gla-300 was significantly lower than that with IDeg treatment (P = 0.021). 2-folds decrease in within-night GV with Gla-300 vs Gla-100 2X Nocturnal GV (mean, SD, CV & MAGE) between-nights was numerically lower with Gla-300 SD: Standard deviation; CV: Coefficient of variation; MAGE: Mean amplitude of glycemic variations. Yu NC. Adv Med. 2019;2019:8587265.
T1D Clamp Study: Gla-300 Has Lower Within-day Variability Vs IDeg-100 Single-center, randomized, double-blind crossover euglycemic clamp study included two parallel cohorts with fixed once-daily morning dose regimens (n=45) 20 % lesser within-day variability with Gla-300 vs IDeg-100 Gla-300 provides less fluctuating steady state PD with more evenly distributed PK vs IDeg-100 in a OD morning dose of 0.4 U/kg/day Deg-100: Insulin degludec 100 U/mL; Gla-300: Insulin glargine 300 Units/mL. Bailey TS, Pettus J, Roussel R, et al. Diabetes Metab. 2018;44(1):15–21.
Time-Below-Range Was Markedly Lower For Gla-300 Comparable TIR for Gla-300 vs IDeg with TBR markedly lower for Gla-300 across categories of hypoglycaemia Kawaguchi Y, et al. J Diabetes Investig. 2019;10(2):343–351. Deg: Insulin degludec; Gla-300: Insulin glargine 300 U/mL.
Poll #5 According to you, which is the most clinically relevant advantage of Gla-300 vs first generation basal insulins to address GV? Lower risk of anytime hypoglycaemia Lower risk of nocturnal hypoglycaemia Longer duration (>24-h coverage) More convenient leading to better adherence Easy and safe titration leading to optimal dose administration Effectively fixing fasting leading to lowering of PPG excursions B. Lower risk of nocturnal hypoglycaemia