Download
1 / 1
10 likes | 121 Views
Baseline quality of life (QOL) is a strong and performance status (PS)-independent prognostic factor for overall survival (OS) in patients with metastatic colorectal cancer (mCRC) A. Grothey 1 , D.J. Sargent 1 , D.W. Szydlo 1 , X. Zhao 1 , M Campbell 1 , R.M. Goldberg 2 , J.A. Sloan 1

E N D
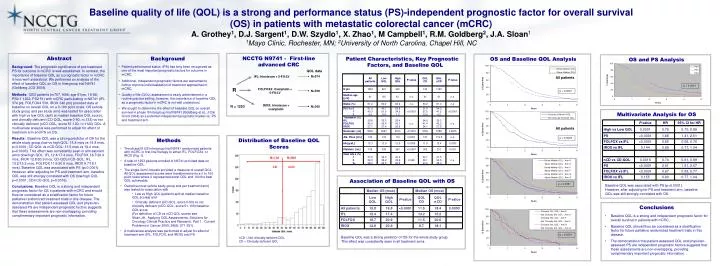
Baseline quality of life (QOL) is a strong and performance status (PS)-independent prognostic factor for overall survival (OS) in patients with metastatic colorectal cancer (mCRC) A. Grothey1, D.J. Sargent1, D.W. Szydlo1, X. Zhao1, M Campbell1, R.M. Goldberg2, J.A. Sloan1 1Mayo Clinic, Rochester, MN; 2University of North Carolina, Chapel Hill, NC NCCTG N9741 - First-line advanced CRC Abstract Background: The prognostic significance of pre-treatment PS for outcome in mCRC is well established. In contrast, the importance of baseline QOL as a prognostic factor in mCRC is less well understood. We performed an analysis of the effect of baseline QOL on OS in Intergroup trial N9741 (Goldberg JCO 2004). Methods: 1253 patients (m767, f486; age 61yrs, 19-88; PS0-1 1202, PS2 51) with mCRC participating in N9741 (IFL 374 pts, FOLFOX4 539, IROX 340 pts) provided data at baseline on overall QOL on a 0-100 point scale. OS (whole study group and per study arm) was tested for association with high vs low QOL (split at median baseline QOL score), and clinically deficient (CD-QOL, score 0-50, n=133) vs not clinically deficient (nCD-QOL, score 51-100, n=1120) QOL. A multivariate analysis was performed to adjust for effect of treatment arm and PS on OS. Results: Baseline QOL was a strong predictor of OS for the whole study group (low vs high QOL: 15.8 mos vs 19.8 mos, p<0.0001; CD-QOL vs nCD-QOL: 11.5 mos vs 18.4 mos, p=0.0003). This effect was consistently seen in all treatment arms (low/high QOL: IFL 12.4/17.4 mos, FOLFOX 18.7/20.9 mos, IROX 12.8/20.9 mos; CD-QOL/nCD-QOL: IFL 13.2/15.2 mos, FOLFOX 11.5/20.6 mos, IROX 8.7/18.1 mos). Baseline QOL was associated with PS (p<0.0001). However, after adjusting for PS and treatment arm, baseline QOL was still strongly correlated with OS (low/high QOL p=0.0001; CD/nCD-QOL p=0.0016). Conclusions: Baseline QOL is a strong and independent prognostic factor for OS in patients with mCRC and should thus be considered as a stratification factor for future palliative randomized treatment trials in this disease. The demonstration that patient-assessed QOL and physician-assessed PS are independent prognostic factors suggests that these assessments are non-overlapping, providing complimentary important prognostic information. • Background • Patient performance status (PS) has long been recognized as one of the most important prognostic factors for outcome in mCRC. • Additional, independent prognostic factors are warranted to further improve individualization of treatment approaches in mCRC. • Quality of life (QOL) assessment is easily administered in a routine practice setting, however, the importance of baseline QOL as a prognostic factor in mCRC is not well understood. • We sought to determine the effect of baseline QOL on overall survival in phase III Intergroup trial N9741 (Goldberg et al., J Clin Oncol 2004) as a potential independent prognostic marker vs. PS and treatment arm. Patient Characteristics, Key Prognostic Factors, and Baseline QOL OS and Baseline QOL Analysis OS and PS Analysis QOL data N=374 IFL: Irinotecan + 5-FU/LV All patients p < 0.0001 R FOLFOX4: Oxaliplatin + 5-FU/LV N=539 p < 0.0001 IROX: Irinotecan + oxaliplatin N = 1253 N=340 Multivariate Analysis for OS All patients Methods Distribution of Baseline QOL Scores p = 0.0003 • The phase III US Intergroup trial N9741 randomized patients with mCRC in first-line therapy to either IFL, FOLFOX4, or IROX (Fig. 1). • A total of 1253 patients enrolled in N9741 provided data on baseline QOL. • The single-item Uniscale provided a measure of overall QOL. AllQOL assessment scores were transformed onto a 0 to 100 point scale where 0 represented worst QOL and 100 the best QOL achievable. • Overall survival (whole study group and per treatment arm) was tested for association with • Low vs High QOL (patients split at median baseline QOL scores) and • Clinically deficient (CD-QOL, score 0-50) vs not clinically deficient (nCD-QOL, score 51-100) baseline QOL score(For definition of CD vs nCD QOL scores see: Sloan JA. Applying QOL Assessments: Solutions for Oncology Clinical Practice and Research, Part 1. Current Problems in Cancer 2005; 29(6): 271-351) • A multivariate analysis was performed to adjust for effect of treatment arm (IFL, FOLFOX, and IROX) and PS. N=102 N=900 CD nCD Association of Baseline QOL with OS Baseline QOL was a strong predictor of OS for the whole study group. This effect was consistently seen in all treatment arms. p < 0.0001 Baseline QOL was associated with PS (p<0.0001). However, after adjusting for PS and treatment arm, baseline QOL was still strongly correlated with OS. • Conclusions • Baseline QOL is a strong and independent prognostic factor for overall survival in patients with mCRC. • Baseline QOL should thus be considered as a stratification factor for future palliative randomized treatment trials in this disease. • The demonstration that patient-assessed QOL and physician-assessed PS are independent prognostic factors suggests that these assessments are non-overlapping, providing complimentary important prognostic information. p < 0.0001 nCD = Not clinically deficient QOLCD = Clinically deficient QOL



















