Download
1 / 46
460 likes | 1.4k Views
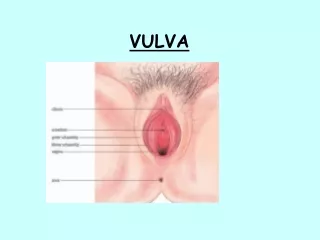
ONCOLOGY OF VULVA AND VAGINA. THE VULVA. INCIDENCE: OVER 400, OVER 200 DETHS (ANNUAL IN POLAND) 40-60% STAGE III and IV – FIGO – inolved lymph nodes.

E N D
INCIDENCE:OVER400, OVER 200DETHS (ANNUAL IN POLAND)40-60% STAGE III and IV – FIGO – inolved lymph nodes
Risk factorslow level of hygiene, HSV, HPV(40%), chlamydia trachomatis,cosmeticsage – organism involution (i.e. metabolic abnormalities)
Prognosis 5-year survivalI (FIGO) - 90%IV (FIGO) - 18%(all togother 35%)
VIN - vulvar intraepithelial neoplasia(SIL –squamos intraepithelial lesion)
VIN 1(low grade dysplasia)– 1/3 lower part of epitheliumVIN 2(intermediary grade dysplasia)– 2/3 lower part of epithelium VIN 3(high grade dysplasia)– 1/3 upper part of epithelium or whole epithelium - ca praeinvasivum or 1/3 lower part similar - ca planoepitheliale G1
Ca planoepitheliale- 90% Bartholin gland Ca - 5%other glandular – Paget disease sarcomas metastatic – breast, kidney, stomach, melanoma
1/3papillar or basal cell carelatively young womenbefore ca – VIN and virus infectionmultifocal
2/3planoepithelial keratodesin older agebefore no VINlichen sclerosusplanoepithelial hyperplasia virus infection rare monofocality
Symptoms - no - itching - pain (clitoris) - abnormalities of defecation and miction - smell secretion
Ways of invasion - infiltration of neighbour structures(urethra, vagina, anus) - metastasis into regional lymph nodes
DiagnositicEVERY disease in region of vulva needs histioathological verification
If melanoma suspection:resection of the whole abnormal tissue with margin of normal tissue
in20% of cases vulvar malignancy coexist with second malignancy of FGT
Stage O(carcinoma in situ, intraepithelial carcinoma)treatment simple resection of vulva local resection
Stage I(tumor infiltrating vulva or perineum; in largest diam max 2 cm; no metastasis to lymph nodes)vulvectomy with bilateral inguinal lymph nodesmargin min.: 8 – 10 mm
If metastasis in lymph nodes – complementary radiation theraphy
In case of patient who does not agree for surgery– radical radiotheraphy
Stage II((tumor infiltrating vulva or perineum; in largest diam over 2 cm; no metastasis to lymph nodes)
Radical vulvectomy (margin of inaffected tissues - min 10 mm)with bilateral inguinal lymph nodes
Complementary radiotheraphy - metastasis in inguinal lymph nodes (2 or more without cossing the capsule of LN or 1 with cossing the capsule of LN or macroscopic invasion)- margin smaller than 8 mm- deph of invassion larger than 5 mm- lymph or capillary vassels invassion
Stopień III(tumor of any size infiltrating urethra, vagina, anus or/and unilateral metastasis to LN)
Deep radical vulvectomy with superficial and profundal inguinal LN, urethraresection, partial resection of anus
Radiotheraphy in patients who can not be qualified to surgery or do not agree
Stopień IVIV A – tu infiltration upper part of urethra, urinal cyst mucose, mucose of anus, pelvic bones, and/or bilateral inguinal LNIV B – distant metastasis including pelvic LN
1. Radical vulvectomy with involved organs (urethra, urinal cyst, anus), with regional LN complementary radiation 2. Radical radiotheraphy 3. Paliative radiation 4. Symptomatic treatment.
Chemotheraphy - as a part of radiochemotheraphy in preoperative radiation in stageIII/IV - in recurence5-fluorouracyl i cisplatin
Ca of vagina – primary - Very rare 1-2% of all FGT cancers 80-90% secondary Planoepithelial ca - (85%) - in this 80% cervical ca, 17% vulva ca Glandular ca - – endometrium (32%), colon (26%), ovary (17%) kidney, breast, chorioncarcinoma
Ethiology of primary ca of vagina • ? • mechanic contraceptives • persistent leukorrhea • leucoplakia • vaginitis • late menopause • masturbation • viral infection • pessars • lack of estrogenes
Location Most frequent - 1/3 – back-upper wall Less frequent - 1/3 low part Sporadic in the middle part of vagina
Symptoms At the beginning – NO In advanced stages – Contact bleeding, leukorrhea, urinal bladder, anus abnormalities
Diagnosis - hist-pat verification of the tumor - colposcopy with biopsy - exclussion of cervical cancer (cervical tissue sections / abrasion) - other cancer than planoepithelial - Uteral cave abrassion, USG, mammography - cystoscopy + tissue sections ( front wall) - rectoscopy + tissue sections ( back wall)
Treatment • Surgery (partly!) • radiotheraphy ! • teleradiotheraphy • brachyteraphy • (chir + rtp) • chemotheraphy (advanced stages) (Cisplatyna, 5Fu, Mitomycyna)
5-year survival average 35 % Iº - 70% - 80% IVº - 0% - 18%