Download
1 / 30
310 likes | 502 Views
The Value of Zero-Hour Implantation Biopsies Volker Nickeleit Nephropathology Laboratory, Department of Pathology The University of North Carolina, Chapel Hill, USA.

E N D
The Value of Zero-Hour Implantation BiopsiesVolker Nickeleit Nephropathology Laboratory, Department of Pathology The University of North Carolina, Chapel Hill, USA
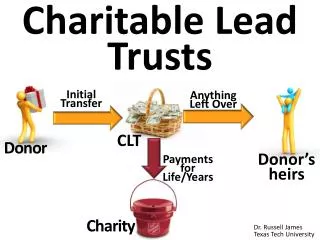
Baseline Renal Allograft Biopsies Purpose: 1) Organ adequacy (Harvest biopsy) 2) Pre-existing Disease (Protocol Biopsy) a) Post transplant biopsy interpretation (“book-keeping”)b) Prediction of function / management c) Diagnosis of (living) donor disease
Donor harvest biopsies Harvest biopsies of limited practical valuePurpose: 1) Organ adequacy : + / - (adjunct tool) 2) Pre-existing Disease : + / -a) Adequate post transplant biopsy interpretation b) Implantation protocol biopsies
Harvest biopsies of limited practical valuePurpose: 1) Organ adequacy : + / - (adjunct tool) 2) Pre-existing Disease : + / -a) Adequate post transplant biopsy interpretation (“book-keeping”)Improvement: a) standardization of technique, i.e. needle cores, deep wedges b) complete tissue evaluation (PAS, trichrome) and material sharing with managing transplant center c) systematic studies of criteria to discard organs
a) Donor harvest biopsies b) Implantation protocol biopsies
Implantation protocol biopsies to assess donor disease • Strengths: • a) full histological evaluation “no time constraints” • b) good assessment of lesions “special stains” • Problems: • a) Risk of complications / bleeding • (caveat: living donations)b) Sampling: 15 gauge needles, only one core, no frozen tissue, subcapsular wedge biopsies
UNC experience with post perfusion biopsiesn=175 kidney transplantsn=114 post perfusion zero-hour biopsies (65% of all organs)n=1 Complication (extended bleeding) 0.9% of all biopsiesBiopsy procedure: biopsy gun, 15 gauge needle, 1 or 2 coresTissue fixation in formalin and fresh frozen collection
Baseline Renal Allograft Biopsies Purpose: a) Diagnosis of (living) donor disease b) Identifying “baseline” histological changesc) Prediction of function / management
Baseline Renal Allograft Biopsies Purpose: a) Diagnosis of (living) donor disease b) Identifying “baseline” histological changesc) Prediction of function / management
N=114 biopsies n=72 cadaveric, n=42 living origin donor age: median 37 yrs (range: 9 – 61 yrs)N=78 (68%) Banff minimal adequacy (> 6 glomeruli and > 1 artery; caveat: often medulla)N=22 (20%) Normal (no arteriosclerosis, no glomerulosclerosis)N=42 (37%) Immunofluorescence analysis N=0 Immuncomplex mediated GN N=0 C4d positivity N=0 Tubular HLA-DR expressionN=0 (0%) Active disease
Histological features (total n=114):Glomeruli median: 14 (range: 0 - 52)Sclerosed Glomeruli > 3 sclerosed glomeruli n=1% Interst. fibrosis 0% n=66, <10% n=31, > 10% n=13% Tub. Atrophy 0% n=84, < 10% n=22, > 10% n=6Arteriolosclerosis (0-4) (0) n=57, (1) n=33, (2) n=10, (3) n=1Intimal sclerosis (0-4) (0) n=45, (1) n=24, (2) n=17, (3) n=4 ATN (0-4) (0) n=0, (1) n=78, (2) n=48, (3) n=14, (4)n=1
Moderate Arteriosclerosis ( Scoring: > 2 / 4 ) 21 / 114 biopsies (18%) 18% of cadaveric organs N= 13 cadaveric organs (mean: 37 yrs, range: 18 – 59 yrs) N= 1 secondary FSGS (cadaveric organ) 19% of organs from living donations N= 8 organs of living origin (mean: 46 yrs, range: 37-54 yrs)
Baseline Renal Allograft Biopsies Purpose: a) Diagnosis of (living) donor disease Unexpected arteriosclerosis (suggestive of hypertension induced damage) in 19% of donors b) Identifying “baseline” histological changes Arteriosclerosis and arteriolosclerosis in 40% of organs
Baseline Renal Allograft Biopsies Purpose: a) Diagnosis of (living) donor diseaseb) Identifying “baseline” histological changes c) Prediction of function / management
Acute rejection - graft failure ( 12 months post transplantation) Multi-organ recipients 4/ 114 (4%) Acute rejection 19/ 110 (17%) Graft failure 5/ 110 (5%) BK-Virus nephropathy 8/ 110 (8%) Lost for follow up 4/ 114 (4%) 40 Patients excluded from functional analyses
Statistical analysisHistological features: % globally sclerotic glomeruli % interstitial fibrosis % tubular atrophy arteriolosclerosis (0-4) arterial intimal sclerosis (0-4) ATN (0-4)Clinical data (during 12 months post transplantation):S-Creatinine: 2 weeks, 1, 3, 6, 12 months post txDelayed graft function: at least 1 episode of HD post txBlood-Pressure: 3, 6, 12 months post txAcute rejection episodesGraft lossDemographic data: Recipient age, sex, race, number of tx Donor age, sex, race Type of donor organ
Statistical analysisHistological features: - % globally sclerotic glomeruli - % interstitial fibrosis - % tubular atrophy - arteriolosclerosis - arterial intimal sclerosis Significantly correlated to one anotherLeading variable: arterial intimal sclerosis
Statistical analysis: Arterial intimal sclerosisA) Arterial intimal fibrosis is correlated with the age of the donorAge in years ( mean + SD) Scoring 0 27,9 + 12.0 Scoring 1 42,7 + 8.3 Scoring 2 44.7 + 11.9 Scoring 3 46,7 + 6.3 p< 0.0001B) Arterial intimal fibrosis is not correlated with donor organ type, donor sex, donor race
Statistical analysis **: Arterial intimal sclerosis Arterial intimal sclerosis * Delay. S-Creatinine (mean + SD) Blood pressure( scoring 0-3 ) Funct. 2 1 3 6 12 3 6 12 % Wks m m m m m m mths 0 n=31 13% 1.27 + .321.25+ .33 1 n=14 14% 1.28 + .461.29+ .392 n=7 0% 1.60 + .431.62+ .40 3 n=2 0% 1.25 + .071.35+ .21 ns ns ns ns p<0.04 ns ns ns nsmild (0-1) n=45 13% 1.27+ .361.26+ .34moderate (2-3) n=9 0% 1.52 + .401.55+ .37 nsns ns p<0,04p<0.02 ns ns ns ns* Biopsies fulfilling minimal adequacy criteria only ** Evaluation of functioning renal grafts without rejection during 12 months
Statistical analysis: ATNA) Acute tubular injury (ATN) is correlated with donor organ typeCadaveric Living donation Scoring 0 4 9 Scoring 1 14 18 Scoring 2 38 10 Scoring 3 11 3 Scoring 4 0 1 p<0.001B) Acute tubular injury (ATN) is not correlated with delayed graft function, acute rejection episodes, arterial hypertension
Statistical analysis **: ATN Acute tub. injury Delay. Function S-Creatinine (mean + SD) ( scoring 0 - 4 ) 2 1 3 6 12 Wks m m m m 0 n=7 1.13+ 0.29 1 n=16 1.66+ .792 n=27 1.82+ 1.31 (3 and 4) n=6 2.17+ 1.35 ns p<0.05 ns ns ns ns ** Evaluation of functioning renal grafts without rejection during 12 months (total n=54)
Baseline Renal Allograft Biopsies Purpose: c) Prediction of function / management Arterial intimal sclerosis: - associated with increased S-Cr 3 and 6 months post tx - associated with donor age ATN: - associated with increased S-Cr 2 weeks post tx
Baseline Renal Allograft Biopsies Purpose: a) Diagnosis of (living) donor disease b) Identifying “baseline” histological changesImpact on diagnoses in post transplant allograft biopsies c) Prediction of function / management
Chronic vascular rejection – versus - pre-existing donor disease Zero-Hour Biopsy: Intimal sclerosis Chronic inactive vascular rejection
Pre-existing donor disease and superimposed vascular rejection: 12 days post transplantation Banff type II rejection: Endothelialitis Donor disease: intimal sclerosis Media
Pre-existing donor disease and superimposed rejection 5 months post transplantation: Arterial intimal sclerosis and chronic active vascular rejection
Calcineurin-inhibitor induced arteriolopathy • versus – • pre-existing arteriolosclerosis Zero-Hour Biopsy: arteriolosclerosis Cyclosporine arteriolopathy
Baseline (Zero-Hour) Biopsies • Important for adequate classification of transplant pathology caveat: fibrosis and atrophy may be donor disease! active and scarred rejection may be superimposed on donor disease! • Prediction on graft function • Some help to detect (living) donor disease • Help for scientific projects (e.g. gene expression analysis post tx, latent viral load measurements etc) Specific diagnoses
Back to the Basics of the “Banff Idea”…. …..Bean Counting.
Banff “Edition” for reporting Donor Disease1) Strongly recommend adequate baseline implantation biopsies2) Separately score and report donor disease (“D”)Dcv (0-3): arterial intimal fibroelastosis with marked multilayering of elastic lamellaeDah (0-3), Dci (0-3), Dct (0-3)Dcg: percentage of globally sclerotic glomeruli3) Post transplantation: - score Banff lesions as usual - specifically comment on previous “D” scores