Download
1 / 31
310 likes | 452 Views
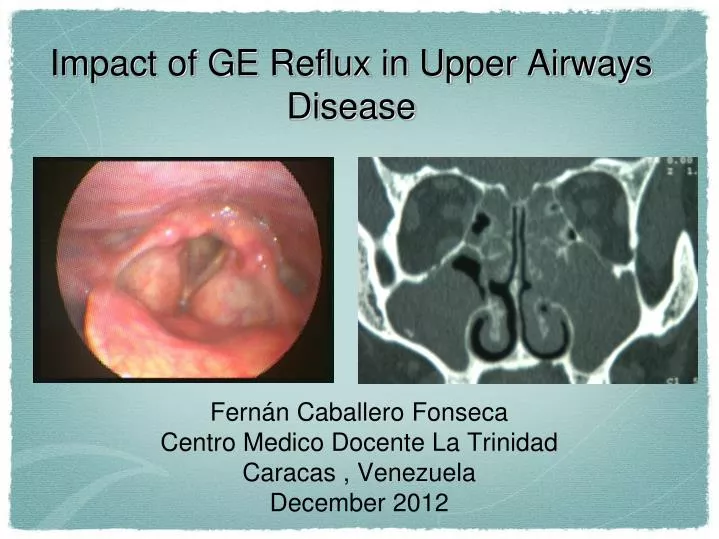
Impact of GE Reflux in Upper Airways Disease. Fernán Caballero Fonseca Centro Medico Docente La Trinidad Caracas , Venezuela December 2012. Reasons to Go to the Doctor. Who has not have a patient with “ frequent throat clearing ”? Who has not have a patient with “Persistent sore throat”?

E N D
Impact of GE Reflux in Upper Airways Disease • Fernán Caballero Fonseca • Centro Medico Docente La Trinidad • Caracas , Venezuela • December 2012
Reasons to Go to the Doctor • Who has not have a patient with “frequent throat clearing ”? • Who has not have a patient with “Persistent sore throat”? • Who has not have a patient with “foreign body sensation ”? • Who has not have a patient with post nasal drip? • Who has not have a patient dysphonic? • Who has not have a patient with “nocturnal awakenings”?
GE RefluxEpidemiology • Gastroesophageal reflux disease (GERD) has become epidemic in the United States and in the developed world. Since 1970, the prevalence of reflux disease has increased 300 percent nationwide. Yearly, GERD accounts for approximately 5 million outpatient visits and close to 100,000 hospitalizations in America. • It is highly prevalent worldwide with a prevalence of 10%-20% in the western world. It is estimated that GERD affects 18.6 million people in the United States. The prevalence of weekly symptoms has increased to an annual rate of approximately 5% in North America. In the US adult population, 10%-20% of people have symptoms at least once weekly and 15%-40% of people have symptoms at least once monthly World J Gastrointest Endosc. 2010 December 16; 2(12): 388–396. Published online 2010 December 16. doi: 10.4253/wjge.v2.i12.388 PMCID: PMC3010469
Pharynx UES Esophagus Cruraldiaphragm Angle of His Pylorus LES Stomach ERGEMechanisms • Transitory relaxation of LES • Increased Intra –abdominal pressure • Decreased oesophagus capacity • Delayed gastric empting
GE RefluxMechanisms Reflux Barrier • 4 components: • - Pressure (intrinsic and extrinsic factors) • - LES length • - Hiatal hernia • - Compliance or yield at the GEJ
Differential Diagnosis • Chonic rhinosinusitis • Funtional dysphonia • Chronic tonsilitis • Sleep apnea • Gastro oesophageal reflux disease GORD or GERD
Common Presenting Symtoms of GERD in Pediatric Patients Infants • Feeding refusal • Recurrent vomiting • Poor weight gain • Irritability • Sleep disturbance • Apparent life-threatening event Older Child/Adolescent • Abdominal pain/heartburn • Recurrent vomiting • Dysphagia • Asthma • Recurrent pneumonia • Upper airway symptoms (chronic cough, hoarse voice) Rudolph CD, Mazur LF, Liptak GS, et al. Guidelines for evaluation and treatment of gastroesophageal reflux in infants and children: recommendations of the North American Society for Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr. 2001;32 Suppl 2:S1-31. Abstract
Associated Conditions • Chronic Rhinosinusitis • Laryngospasm • Granuloma • Chronic laryngitis • Subglotic stenosis • Laryngeal cancer • Chronic otitis media Swiss Med Wkly .2012;142w13544
Is There Evidence to Link Acid Reflux with Chronic Sinusitis or any Nasal Symptoms ? A Review of the Evidence. • Poor evidence of cause-effect relationship • There are not good randomized controlled trials available. • The few adult studies are small case-control with moderate levels of potential bias. • There is not enough evidence to consider anti-reflux therapy in adults refractory CRS . Flook EP, Kumar BN. Rhinology. 2011 Mar;49(1):11-6.
Symtoms Attributed to Laryngopharingeal Reflux • Hoarseseness Post nasal drip • Dysfagia Laryngospasm • Dysfonia • Sore or burning throat • Excessive throat clearing • Chronic cough • Globus
Gastroesophageal Reflux Disease and Chronic Sinusitis: In Search of an Esophageal-nasalReflex. • Gastroesophageal reflux and chronic rhinosinusitis . • Chloridic acid and saline solution. • Mucus production , nasal symptom scores and nasal peak flow. • Nasal - esophageal reflex. Wong IW, Rees G, Greiff L, Myers JC, Jamieson GG, Wormald PJ. Am J Rhinol Allergy. 2010 Jul-Aug;24(4):255-9.
Proton Pump Inhibitor Therapy Improves Symptoms in Postnasal Drainage • 75 patients randomized , double blind patients. • Lanzoprazole Vs placebo • Post nasal drip • 50% improvement with Lanzoprasole Vs 5% Placebo Durmus R, Naiboglu B, Tek A, Sezikli M, Cetinkaya ZA, Toros SZ, Eriman TM, Egeli E .ActaOtolaryngol. 2010 Sep;130(9):1053-7.
An Approach to the Management of Paroxysmal Laryngospasm. • 15 patients ; 9 females and 6 men • Average age 56 +/- 6 years. • 80% associated to to GERD. • Treated with PPI • 6 total improvement, 4 partial improvement and 5 did not respond. Obholzer RJ, Nouraei SA, Ahmed J, Kadhim MR, Sandhu GS.J Laryngol Otol. 2008 Jan;122(1):57-60.
Vocal CordDysfuntion Symptoms Cough Dispnea Dysphonia Estridor Weezing Dysfagia Anxaiety
GERD and VCD • Powell et al. (2000) • 22 patients (age <18) with VCD • 21/ 22 patients with severe aritenoid oedema and congestion during endoscopy . • Loughlin et al. (1996) • 12 adult patients with VCD • 11/ 12 patients with laringytis during endoscopy • 10/12 with abnormal PH-24hs • All patients responded to anti reflux therapy with total improvement of the VCD syptoms.
GERD and VCD Cukier-Blaj et al.:Laryngoscope 118: February 2008
Otologic Findings in Children with Gastroesophageal Reflux. • 73 children ( average 13 months.). • Fail AE , timpanogram curves B, and one or two sighs of GERD . • 40 treated children , 29 not treated 4 no follow up . • 52,5% resolution Vs 45% in the control group ,and by 40% improvement Vs 30% on the control group. Int J PediatrOtorhinolaryngol. 2007 Nov;71(11):1693-7. Serra A, Cocuzza S, Poli G, La Mantia I, Messina A, Pavone P.
Multicentric study: statistical correlation between clinical data and instrumental findings in laryngo-pharyngeal reflux: proposal for a new ENT classification of reflux CA Leone and F Mosca Acta Otorhinolaryngol Ital. 2006 October; 26(5): 264–270
Multicentric study: statistical correlation between clinical data and instrumental findings in laryngo-pharyngeal reflux: proposal for a new ENT classification of reflux Grade A :Erythema/Oedema back and/or lateral regions; Grade B :Erythema/Oedema back and/or lateral and front regions; Grade C:Erosion/Granulation back and/or lateral regions; Grade D:Erosion/Granulation back and/or lateral and front regions. CA Leone and F Mosca ActaOtorhinolaryngol Ital. 2006 October; 26(5): 264–270
Clinical and Phmetric Evaluation ofGastro-esophageal Reflux Impact on Upper Airways in Adult • 95 patients evaluation clinical parameters Vs phmetric findings. • Positive correlation in 81,2% of the patients. • Ulcers 80%, leucoplasias 71,4% y granulomas 100% of phmetrics positives. Sethom Anissa, Khemaies Akkari, Khaled Riahi, Imed Miled, Sonia Benzarti, Mohamed Kamel ChebbiLa tunisie Medicale - 2012 ; Vol 90 ( n°03 ) : 243 - 247
Role of Rhinitis in Laryngitis: Another Dimension of the Unified Airway. • 134 AR patients, 54 Non allergic rhinitis , and 62 controls. • Prevalence de dysphonia: 32.8% AR, 26.9% NAR y 8.1% controls (P<0,001) • Odds ratio, 4.22; 95% confidence interval compared with Asthma, GE reflux and inhaled corticoid usage . Turley R, Cohen SM, Becker A, Ebert CS Jr.AnnOtolRhinolLaryngol. 2011 Aug;120(8):505-10.
Diagnosis • Pharyngeal –laryngeal symptoms. • Post nasal drip. • Indirect laryngoscope and posterior rhinoscopy. • Video endoscopy .
Final thoughts • The GE reflux is a very common disease and its prevalence seems to be growing. • It has direct relationship with many entities in the ENT area . • By large is a clinical diagnosis but many patients may lack GI symptoms , para clinical evaluation may help in some patients. • Many patients, but not all, will improve with anti reflux therapy. • The PPI trial may be useful toll as diagnosis and treatment in many patients with GERD.