Download
1 / 15
150 likes | 284 Views
Access To Emergency Care. Prepared by: Alison Haddock, MD University of Michigan. “I mean, people have access to health care in America. After all, you just go to an emergency room.” President George W. Bush July 2007. Safety Net. EDs are obligated to provide care to all

E N D
Access To Emergency Care Prepared by: Alison Haddock, MD University of Michigan
“I mean, people have access to health care in America. After all, you just go to an emergency room.” President George W. Bush July 2007
Safety Net • EDs are obligated to provide care to all • Federal law (EMTALA ) in 1986 • Requires examination and treatment of all patients, regardless of ability to pay • No funding provided
Safety Net • Underinsured and uninsured • Increasing difficulties in obtaining access to primary care • Multiple barriers • Lack of evening and weekend availability • Difficulty accessing overworked providers • Decreasing reimbursements for PCPs • Providers unwilling / unable to provide uncompensated care
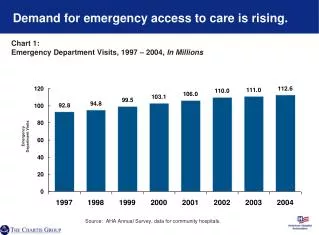
Demand for Services • More than 120 million ED visits anticipated in 2009 • Declining number of inpatient hospital beds • Closure of public hospitals • All hospitals under increasing financial strain • Leads to crowding • Long wait times • Ambulance diversion
Crowding • More patient visits, fewer EDs • Patient outcomes worsened by crowding • Increased time to physician for critically ill patients • Increasing numbers of patients “Left Before Being Seen” • Increasing medical errors
Crowding • Admitted patients held in EDs due to lack of inpatient beds • 2002 Lewin Group study: 90% of Level I trauma centers with >300 beds were operating at or above capacity • Improvement requires hospital-wide coordination
At the “Breaking Point” • Institute of Medicine report released in 2006 • Three main conclusions: • EDs are overcrowded. • EMS systems are fragmented. • Many EMS systems and EDs are not well equipped to handle pediatric care. • Recommendations: • End ED boarding and ambulance diversion. • Improve EMS coordination. • Enhance pediatric presence throughout emergency care.
Disparities • Rural Areas • 30% of the population resides more than 30 minutes away from the nearest ED • Rural EDs are less likely to be staffed by EM-trained MDs • 21% of the US population lives rurally; only 12% of emergency physicians live in rural areas
Disparities • Race/Poverty • Increasing difficulties obtaining primary care • Fewer physicians accepting Medicaid as reimbursement declines • More reliance on closing and strained urban public hospitals • Treatment, wait times and insurance authorization appear to vary based on race and ethnicity of patient
Emergency Physician Shortages • Demand for EM-trained doctors exceeds supply • 40% of practicing ED physicians are not EM board-certified or EM residency trained • Not anticipated to change in near future
On-call Specialist Shortage • 73% of ED medical directors reported inadequate specialist coverage in 2005 • Specialists shifting away from hospital practice • Not mandated to provide unreimbursed care • Experiencing increasing demand for their services, improved bargaining power through groups • Providing emergency services leads to increased medical liability exposure
Reform • Nationwide System Change • 68% of EM physicians surveyed in 2008 supported a plan to institute a national health insurance program • Access to EMS Act • Legislation introduced in 2007 and 2009, currently pending • Calls for further investigation of causes and solutions to crowding and diversion • Would improve physicians payments for services provided under EMTALA
Future Directions • More details on many important issues discussed in future presentations • Become an advocate! • Sign up for ACEP’s 9-1-1 network • Call or email your congressional representatives • Share information in local organizations and publications