Download
1 / 23
230 likes | 357 Views
Conditional Cash Transfers for Improving Utilization of Health Services. Health Systems Innovation Workshop Abuja, January 25 th -29 th , 2010. Conditional Cash Transfers (CCTs).

E N D
Conditional Cash Transfers for Improving Utilization of Health Services Health Systems Innovation Workshop Abuja, January 25th-29th, 2010
Conditional Cash Transfers (CCTs) • Cash transfers are conditioned when in addition to satisfying a selection criteria, beneficiaries are required to regularly undertake some pre-specified action • CCTsGovernment programs that transfer cash to poor families on the condition that those families make investments in human capital, usually: • Sending children to school regularly • Taking children to regular health and nutrition check ups
For example –Colombia • The program transfers about US$40 per month (about 30% of household consumption) to extremely poor families with children less than 18 living in rural areas • To receive the transfers: • Children 6-18 have to attend school regularly (85%) • Children less than 6 have to be taken to health centers every two (0-1) or six months (2-5). • Transfer has two parts: • A single transfer if the family has children less than 5 • Additional transfers for every school age child
Objectives • Two broad objectives: • Short-term: support household consumption/income protection • Mid-term: accumulate human capital and break the intergeneration transmission of poverty • Specific objectives depend on the defined sector goals (e.g., schooling, health status, nutrition)
Rationale • Cash Transfers to • Help poor families to access basic services • Create incentives to change behaviors • CCTs reach their long-term goals by boosting demand for specific social services • Therefore, CCTs make sense only if supply of social services is available for, and reachable by beneficiaries
….help them to improve their consumption • Colombia: higher consumption of proteins (milk, meat, eggs) and cereals; and children cloths. No evidence of additional consumption of alcohol or goods for adults • In Brazil, 60% of the transfer spent in food; in 75% of families enhanced variety of food, increased the number of meals, and improved quality of food (more proteins).
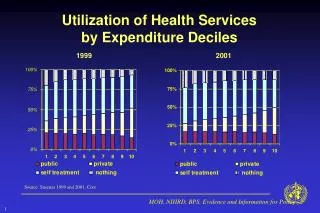
CCTs assisted families to use health facilities for their children… • Growth monitoring check ups • México (+30-60%), Nicaragua (29%), Honduras (+12-20%), Colombia (+23-30%) • Visit to clinics • Colombia: (+30% (0-2), +50% (2-4)), Honduras (+20%) • Pre-natal check ups: • México (+6%), Honduras (+19%), Brazil (+6%)
…helping to reduce stunting… • In México, beneficiary children are 1cm taller than non-beneficiaries after 2 years • In Colombia and Nicaraguastunting among beneficiaries is 6.9 and 5.3 percentage points lower • In Brazil, after two years of exposure to BolsaFamiliabirth weight is approximately 200 gms more among beneficiaries.
… and increase immunization coverage • Colombia: +9% (DPT3) • Honduras: +7% (DPT3) • Nicaragua: +18% (full) • Turkey: +14% (full) (difference between beneficiaries and non-beneficiaries)
Beneficiaries receive payment Program authorizes payments Key implementation issues: TheCCTbasiccycle Beneficiaries comply with conditions Program objectives and expected outcomes Define target population Selection of beneficiaries Program monitors and verify compliance Registry of beneficiaries (and information system) Define conditionalities
Targeting • Selecting beneficiaries of the program • Depends on the objectives of the program and the conditions • Windows of opportunities • How • Geographical • At household level (Proxy means tested) • Community participation
Conditionality • Simple • Easy to understand by beneficiaries • Easy to monitor • Linked to transfer
Registry of Beneficiaries • At the core of the program • Data base with all the information of all beneficiaries (surveys) • Needs to be updated • Basis for monitoring compliance with conditions and authorizing payments
Verification of conditionalities • Central issue to a CCT program • May be difficult and expensive, but critical for the credibility and impact of the program • Close coordination between Ministries and implementing agencies • Following and support to families that fail to comply
Information • CCT programs require a careful management of information • Large CCT programs require to manage considerable amount of information regularly (e.g., Brazil -10m payments per month; Mexico: 5m payments every two months) • Information of compliance with conditions • Information on non-compliant families
Benefits and payments • Single transfer per family or per eligible member • High enough to be an incentive • Low enough to avoid interfering in household decisions on labor options • Frequency is key to keep families aware of conditionality and change behaviors • Clear definition and application of consequences for families that fail to comply
Other implementation issues • Institutional coordination (horizontal and vertical) • Transparency in the operation: using banking system to transfer cash to families • Community feedback • Monitoring and evaluation to adjust program • Exit and link with other strategies
Gradual expansion • Most programs started from small and simple interventions… • Only selected areas • Straightforward and simple conditions • Categorical targeting • … for several reasons… • Lack of supply of social services, • Institutional capacity at central and local level • Adjust the program and ensure credibility • … and nationwide expansion is a mid-term process (if at all)
Size of the program Annual program budget as % of GDP
Amount of the benefit % of household consumption
Concluding remarks • Start simple but complete • CCT instruments to reach its goals • Targeting • Conditionalities • Benefits • Critical elements • Available supply of services • Regular monitoring of compliance • Information