Download
1 / 27
270 likes | 588 Views
The Shoulder. Introduction. Components of the shoulder Most common joint pathology Rotator cuff Biceps Tendon Fractured neck of Femur Dislocation Adhesive Capsulitis. 3 components. The glenohumeral joint The acromiclavicular joint The scapular. Diagnosis. History Range of Movement

E N D
Introduction • Components of the shoulder • Most common joint pathology • Rotator cuff • Biceps Tendon • Fractured neck of Femur • Dislocation • Adhesive Capsulitis
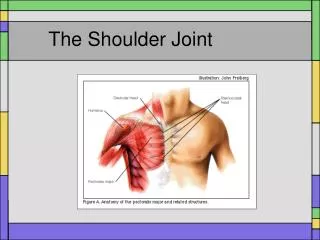
3 components • The glenohumeral joint • The acromiclavicular joint • The scapular
Diagnosis • History • Range of Movement • Palpation • Pain • Diagnostic tests (there are 65 that can be performed!)
Shoulder or cervical nerve root? • Is there loss of shoulder ROM? YES = SHOULDER • Are the reflexes reduced? YES = CERVICAL
Rotator Cuff • Stabilise the head of the humerus while the other major muscles around the shoulder are actively moving the arm. Eg. When deltoid is abducting. They also initiate most movements
3 main types of rotator cuff lesions • Tendonitis • Partial rupture • Complete rupture
Rotator Cuff strengthening Sidelying Lateral Rotation
Rotator Cuff strengthening Prone Horizontal Abduction
Rotator cuff strengthening Lateral rotator strengthening with resistance band
Fractured neck of femur • Pain on early movement • Upper arm swelling • Need to be investigated early especially following a fall in the elderly • Should be kept moving as much as possible
Ghjt disclocation • Carries a very specific history of trauma - anterior dislocation (abduction, extension and lateral rotation) • Usually involves tear of labrum • Physio aims to strengthen rotator cuff • After 3rd dislocation surgery is usually necessary
Adhesive Capsulitis/Frozen shoulder • inflammation of the shoulder capsule and synovial membrane leading to adhesion formation. This causes a thickening in the capsule and constriction of the glenohumeral joint due to the scar tissue forming in the capsule
Diagnosis • Age 40+ • Cause ? Unknown Possible: trauma, wrench, dislocation. CVA, heart conditions, diabetes, viral. Can also be secondary to cx spondylosis or to tendonitis.
Clinical features • Increasing dull ache over a few months duration. • Sharp pain when reaching the end of pain free movement • Loss of movement in a capsular pattern – lateral rotation – abduction - flexion Most reduced >>>>>>>>>Least reduced • Elevation and protraction of shoulder girdle
Clinical features cont’ • Pain over A/C joint and deltoid muscle – can spread to neck and/or elbow • All G/H movement often painful, not specific planes • Pain worse at night
Clincial features cont’ • Muscle spasm in pectoralis major and latissimus dorsi • Wasted deltoid • Associated posture • Dowagers hump • Poke chin
Prognosis • 18 months to 3 years 3 phases • Freezing –painful phase (worse at night and when lying on it) • Frozen – stiff phase • Thawing- stiffness gradually eases
Physiotherapy • Reduce pain with electrotherapy, TENS and acupuncture until patient is able to sleep and function day to day • Taping to rest the joint • Static strengthening exercises for the shoulder • Introduce stretching in sub acute phase
Other treatment • Antiinflamatories • Muscle relaxants • Hydrocortisone injection • Nerve block • Surgery – Manipulation/Arthroscopic capsular release