Download
1 / 25
320 likes | 685 Views
Neurotransmitters and Pharmacology. Mindy M. Escobar Argyle V. Bumanglag September 20, 2007. Neurotransmission. Why is it important to regulate the amount of neurotransmitter present in the synapse?. Serotonin. Plays an important role in regulation of: Aggression Appetite

E N D
Neurotransmitters and Pharmacology Mindy M. Escobar Argyle V. Bumanglag September 20, 2007
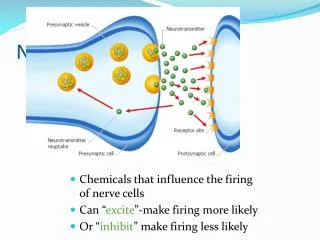
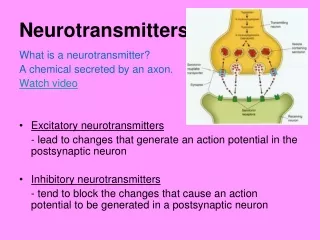
Why is it important to regulate the amount of neurotransmitter present in the synapse?
Serotonin Plays an important role in regulation of: Aggression Appetite Body temperature Sleep Vomiting Mood Sexuality Anger
Principle source of serotonin Raphe nuclei
Psychedelic serotonin modulation Mood, thought processes and concentration Appetite Psychomotor control and perception Emotional responses
Hallucinogens (LSD) • Serotonin antagonist • Completely blocks activity of Raphe nuclei • Results in disinhibition of critical control systems over sensation, sleep, attention, and mood
MDMA (ecstasy) • Increases serotonin release and blocks reuptake • Enhances communication, reduces psychological defenses, and increases capacity for introspection • Significant risk for chronic physical harm
Therapeutic serotonin modulation www.psychiatrist.com/pcc/brainstorm/br6305.htm
Tricyclics Examples: Vivactil, Elavil, Norpramin, Asendin, Anafranil
SSRIs Examples: Prozac, Paxil, Zoloft, Lexapro, Celexa
Dopamine Synthesis Pathway (1) Pre-synaptic DA neuron (2) (3) (6) DA Transporter (4) (5)
Dopamine Receptors • All DA receptors are G-protein-coupled metabotropic receptors • There are 5 subtypes of dopamine (DA) receptors that can be grouped into 2 main classes: D1 and D2 receptors • D1 receptors include subtypes D1 and D5 • D1 receptors are the most abundant and widespread in areas receiving DA innervation • D1 receptors mediate peripheral effects - renal vasodilatation and increased myocardial contractility • D2 receptors include D2,D3, and D4 • Antipsychotic drugs show a high affinity for the D2 receptors, which may play a role in schizophrenia • D3 receptors found on the presynaptic terminal act to inhibit DA synthesis and release
Dopamine Pathways 3 Major Pathways in the CNS (1) Nigrostriatal system • Motor control (2) Mesolimbic/mesocortical pathway • Behavioral effects (3) Tuberohypophyseal system • Endocrine control (2) (1) (3)
Cocaine • Derived from the leaves of the coca plant, which grows in some South American Countries • One of the major psychostimulants of abuse • Mechanisms of Action • produces massive release of dopamine into the synaptic cleft • blocks the neuronal re-uptake transport system for catecholamines (DA, NE, 5-HT) • euphoric effects are due to its effects on DA • Other uses • medical use as a local anesthetic Coca plant
Cocaine: Effects • Psychomotor effects (DA mediated) • Euphoria • Increased motor activity • Magnification of pleasure • Peripheral effects • Tachycardia • Vasoconstriction • Increased blood pressure • Adverse effects • Hypertension • Vasospasm of arteries • Myocardial infarcts • Stroke • Impaired brain development in utero • High risk for dependency
Dopamine Reward Pathways http://thebrain.mcgill.ca
Parkinson’s Disease • Parkinson’s Disease is a chronic movement disorder first described in 1817 by James Parkinson • It typically starts around the age of 60, although 5-10% exhibit signs before the age of 40 • Clinical symptoms • Usually begins with a slight tremor or stiffness involving an arm or leg on one side of the body • Prominent tremor at rest and occurs at a frequency of 3-6 per second • Pill rolling • Limb rigidity • Akinesia • Bradykinesia • Characteristic gait, drooling, eye blinking, and a frozen facial expression
Parkinson’s Disease • Clinical manifestations are caused by a network dysfunction of the basal ganglia • In the normal brain, DA projections from the substantia nigra maintain normal function in basal ganglia • Degeneration of DA neurons in the substantia nigra removes a DA-mediated inhibition that makes normal movement possible • Clinical signs begin when approximately 40% of DA neurons have died and approximately 50% of the DA in axon terminals of the basal ganglia has been depleted
Anatomy of the Basal Ganglia www.dana.org
Parkinson’s Disease http://www.urmc.rochester.edu/neuroslides/slide199.html
Treatment of Parkinson’s Disease • Goal of therapy • Restore the deficit in DA receptor function • Inhibit muscarinic cholinergic receptors • Drugs used in treatment of Parkinson’s Disease • Levodopa • Most widely used form of therapy for Parkinson’s Disease • Converted to DA, thereby restoring concentration of DA at the basal ganglia • DA receptor agonists • Mimics the effects of endogenous dopamine • Less effective than levodopa • Monoamine (MAO) inhibitors • Inhibition of MAO increases DA concentration within cells and at the postsynaptic receptor • Muscarinic cholinergic receptor antagonists • Affect the tremor more than the rigidity and hypokinesia • Amantidine • Antiviral drug that was accidentally found to have anti-PD effects • Mechanism uncertain but probably increases endogenous DA