Download
1 / 16
160 likes | 308 Views
Which of the following is/are true regarding Ulcerative Colitis (UC)? A. Females are affected more then males. B. Surgery is curative. C. The most consistent risk factor is family history. D. 75% of patients with Crohn’s will be have a positive p-ANCA antibody, distinguishing it from UC.

E N D
Which of the following is/are true regarding Ulcerative Colitis (UC)? A. Females are affected more then males. B. Surgery is curative. C. The most consistent risk factor is family history. D. 75% of patients with Crohn’s will be have a positive p-ANCA antibody, distinguishing it from UC. E. Smokers are at a higher risk for developing UC.
Which of the following is/are true regarding Ulcerative Colitis (UC)? A. Females are affected more then males. (FALSE - approximately equal in both genders) B. Surgery is curative. (TRUE) C. The most consistent risk factor is family history. (TRUE) D. 75% of patients with Crohn’s will be have a positive p-ANCA antibody, distinguishing it from UC. (FALSE - UC patients are p-ANCA Ab +) E. Smokers are at a higher risk for developing UC. (FALSE - Active smokers are at a lower risk)
Which of the following is a feature of UC, Crohn’s, or both? • segmental disease (skip lesions) • transmural involvement • granulomas • cancer risk • small bowel involvement • “cobblestoning” • rectal disease • bleeding per rectum • diarrhea • infiltration of PMNs into the crypts of Lieberkuhn forming crypt abscesses
Which of the following is a feature of UC, Crohn’s, or both? • segmental disease (skip lesions) (Crohn’s) • transmural involvement (Crohn’s) • granulomas (Crohn’s) • cancer risk (both) • small bowel involvement (Crohn’s) • “cobblestoning” (Crohn’s) • rectal disease (both) • bleeding per rectum (both) • diarrhea (both) • infiltration of PMNs into the crypts of Lieberkuhn forming crypt abscesses (UC)
Which of the following is/are TRUE about the pathologic features of UC? A. UC always involves the rectum. B. UC patients may have pancolitis but it usually stops at the hepatic flexure. C. Strictures are usually caused by malignant transformation of the muscularis mucosa. D. UC involves only mucosa and submucosal layers. E. UC may progress to toxic megacolon with risk of necrosis and perforation.
Which of the following is/are TRUE about the pathologic features of UC? A. UC always involves the rectum. (TRUE) B. UC patients may have pancolitis but it usually stops at the hepatic flexure. (FALSE, splenic flexure) C. Strictures are usually caused by malignant transformation of the muscularis mucosa. (FALSE, benign strictures) D. UC involves only mucosa and submucosal layers. (TRUE) E. UC may progress to toxic megacolon with risk of necrosis and perforation. (TRUE)
Name some of the extraintestinal manifestations of IBD that commonly occur in UC.
Name some of the extraintestinal manifestations of IBD that commonly occur in UC. • ankylosing spondylitis • primary sclerosing cholangitis (more common in UC) • erythema nodosum (more common in Crohn’s) • pyoderma gangrenosum (more common in UC) • uveitis • sacroiliitis
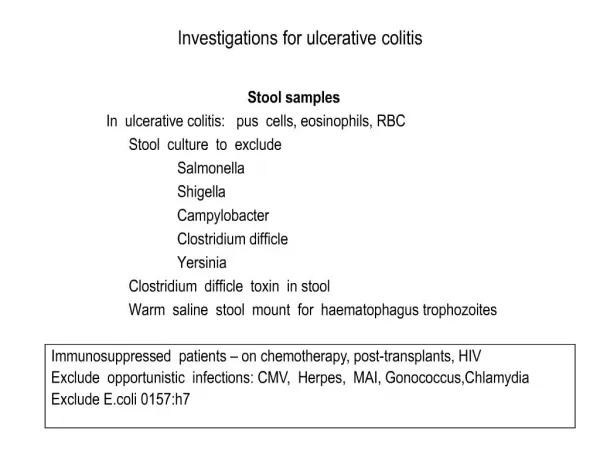
Which of the following is/are true? A. The test of choice for diagnosis of UC is a barium enema. B. All patients with newly diagnosed UC should have an UGI series with small bowel follow through. C. The risk of carcinoma is directly related to the duration of disease and is 50% 40yrs after presentation of pancolitis D. Colonoscopic surveillance should be started at least 10 years after diagnosis
Which of the following is/are true? A. The test of choice for diagnosis of UC is a barium enema. (FALSE, colonoscopy) B. All patients with newly diagnosed UC should have an UGI series with small bowel follow through. (TRUE, to rule out Crohn’s) C. The risk of carcinoma is directly related to the duration of disease and is 50% 40yrs after presentation of pancolitis. (FALSE, risk after 40yrs is 75%) D. Colonoscopic surveillance should be started at least 10 years after diagnosis (TRUE)
Name some indications for surgical intervention in UC. • Intractability • Dysplasia-Carcinoma • Massive Colonic Bleeding • Toxic Megacolon
1. Ileal pouch anastomoses + anal mucosectomy 2. Total abdominal colectomy w/ileal rectal anastomosis 3. Total proctocolectomy w/ileostomy 4. IPAA w/stapled anastomosis + diverting ileostomy Match the following operations with ideal candidate: A. > 65 years old and/or decreased fecal continence B. < 65 and proctitis w/rectal dysplasia C. < 65, no rectal dysplasia, but high operative risk D. < 65, no rectal dysplasia, and low operative risk
1. Ileal pouch anastomoses + anal mucosectomy 2. Total abdominal colectomy w/ileal rectal anastomosis 3. Total proctocolectomy w/ileostomy 4. IPAA w/stapled anastomosis + diverting ileostomy Match the following operations with ideal candidate: A. > 65 years old and/or decreased fecal continence B. < 65 and proctitis w/rectal dysplasia C. < 65, no rectal dysplasia, but high operative risk D. < 65, no rectal dysplasia, and low operative risk
Which of the following is/are TRUE regarding post-op complications in the pouch procedure (restorative proctocolectomy)? A. Mechanical bowel obstruction often occurs secondary to dietary indiscretions w/high roughage intake. B. Pouchitis occurs in up to 50% of patients. C. Ceftriaxone is the antibiotic of choice used to treat pouchitis. D. Anal strictures less then 10mm should be dilated. E. Although complication rates are high with the ileal pouch-anal anastomoses procedure, patient satisfaction is also very high.
Which of the following is/are TRUE regarding post-op complications in the pouch procedure (restorative proctocolectomy)? A. Mechanical bowel obstruction often occurs secondary to dietary indiscretions w/high roughage intake. (TRUE) B. Pouchitis occurs in up to 50% of patients. (TRUE) C. Ceftriaxone is the antibiotic of choice used to treat pouchitis. (FALSE, flagyl is preferred) D. Anal strictures less then 10mm should be dilated. (FALSE, less then 5mm) E. Although complication rates are high with the ileal pouch-anal anastomoses procedure, patient satisfaction is also very high. (TRUE)