Download
1 / 10
150 likes | 498 Views
Polycystic ovary syndromE. A common female endocrine disease. SBI4U-01 Mr. Gajewski Bashour Yazji Jason Antrobus Narayan Wagle. Key Terms (things you should know). PCOS – Polycystic Ovarian Syndrome NIH – National Institute of Health

E N D
Polycystic ovary syndromE A common female endocrine disease SBI4U-01 Mr. Gajewski BashourYazji Jason Antrobus Narayan Wagle
Key Terms (things you should know) • PCOS – Polycystic Ovarian Syndrome • NIH – National Institute of Health • NICHD – National Institute of Child Health and Human Development • Anovulation – The absence of ovulation due to immaturity, post-maturity, pregnancy, oral contraceptive pills or dysfunction of the ovary. • Oligomenorhhea – A menstrual cycle greater than 35 days. • Amenorhhea – A menstrual cycle greater than six months. • Prolactin – Hormone that stimulates milk production after childbirth • FSH – Follicle Stimulating Hormone • Estradiol – One of the primary female reproductive hormones, derives from estrogen • Dominant Follicle – The large cyst (which explodes) in the ovary during each menstrual cycle. • Hirsutism – A male pattern of hair growth • Hyperandrogenism: Excessive production of androgens
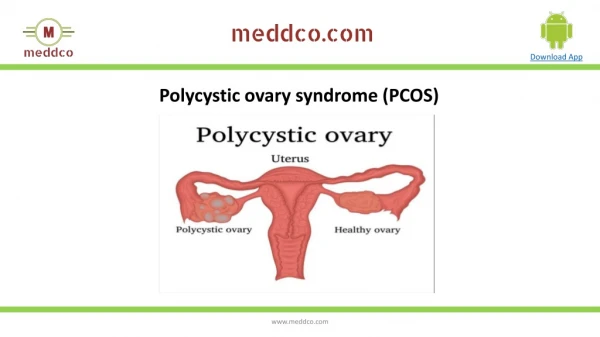
What is the disease? • Polycystic Ovarian Syndrome is one of the most frequent female endocrine disorders. Though scientists are not certain about its origins, most signs point to it being a genetic disease. Between five and ten percent of women of reproductive age (12-45 years) show symptoms such as anovulation (amenorrhea or oligomenorhhea). • Polycystic Ovarian Syndrome was officially discovered in 1990 through a consensus workshop that was sponsored by the NIH and the NICHD in an effort to determine when a patient can be diagnosed for certain with the disease. • The common feature between all diagnoses of PCOS is arrested follicular development. It is believed that the small ovarian follicles are the result of disturbed ovarian function because of failed ovulation, which is displayed by the unreliable menstruation that the condition generally shows.
Causes of PCOS • Though PCOS does not have one specific cause, PCOS is commonly found in women diagnosed with anovulation, among other causes. The World Health Organization criteria for classification of anovulation consists of the diagnosis of oligomenorhhea, which is when the menstrual cycle is greater than 35 days, or amenorhhea, where the menstrual cycle itself is greater than six months in length, as well as a concentration of prolactin, FSH and estradiol. • In a normal menstrual cycle, a dominant follicle bursts in order to release an egg. In PCOS, a condition is developed called follicular arrest, where several follicles develop to a size of 5–7 mm, but not further. No single follicle ever reaches the preovulatorysize, which is 16mm or more.
Signs and symptoms of Pcos • PCOS can be diagnosed through the observation and diagnosis of many varied subsymptoms with varying degree of mildness and severity that affect the reproductive, endocrine and metabolic functions.The three symptoms most commonly found together during the diagnosis of the disorder are hirsutism, menstrual dysfunction, and obesity. Some common symptoms of PCOS include: • Menstrual Disorders: PCOS mostly produces oligomenorrhea or amenorrhea, but other types of menstrual disorders may also occur. • Infertility: Generally results directly from chronic anovulation. • Hyperandrogenism: The most common signs are acne and hirsutism, but it may produce some other symptoms. About three-quarters of patients with PCOS (according to the diagnostic criteria of NIH/NICHD 1990) have evidence of hyperandrogenism. • Insulin resistance is also found to be higher in women with PCOS.
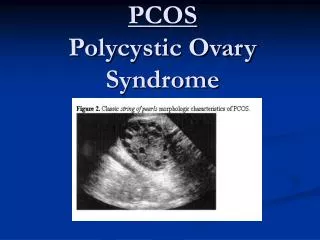
Pathogenesis of PCOS • Polycystic ovaries develop when the ovaries are stimulated by the anterior pituitary to produce excessive amounts of male hormones (androgens), particularly testosterone, by either the release of luteinizing hormone or excessive levels of insulin in the blood, but these two conditions are almost certainly combined with a genetic weakness to the disease, perhaps through family relations. • The syndrome acquired its name due to the common discovery during ultrasound examination of multiple ovarian cysts. These "cysts" are actually immature follicles, not cysts. The follicles have begun to develop, but the development has stopped ("arrested") at an early stage due to the disturbed ovarian function. • Women with PCOS have higher GnRH, which results in an increase in LH/FSH ratio. • As discussed in the last slide, a resistance to insulin (very common in PCOS –positive patients) contributes to LH over FSH dominance, and increased ovarian androgen production anddecreased follicular maturation, all of which contribute to the development of PCOS.
Treatment of pcos • How PCOS is treated varies based on the goals of the patient. Broadly, based on their conditions, they may have one of four goals: • Lowering of insulin levels, restoration of fertility, Treatment of hirsutismor acne, or restoration of regular menstruation. There is some debate as to which treatment is the most effective, especially since there have been no large scale clinical trials comparing them. However, the most effective method to target the underlying cause is a program geared towards weight loss or reduction of insulin resistance, mainly because that’s believed to be the underlying cause. One other popular method of treatment is ovarian drilling, where holes are drilled into the ovaries, through which the immature, stagnant follicles are removed. This method has also seen a lot of success in clinics worldwide.
References and citations • http://www.womenshealth.gov/publications/our-publications/fact-sheet/polycystic-ovary-syndrome.cfm • http://www.medicinenet.com/polycystic_ovary/article.htm • http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001408/ • http://kidshealth.org/teen/diseases_conditions/sexual_health/pcos.html • http://en.wikipedia.org/wiki/Polycystic_Ovarian_Syndrome