Download
1 / 37
370 likes | 501 Views
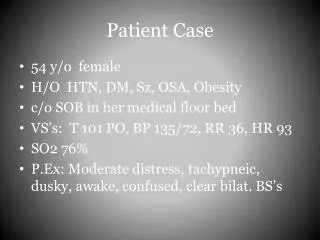
General Anaesthesia and Day-case Patient Anxiety. D r. Mark Mitchell Faculty of Health and Social Care University of Salford Manchester England. m.mitchell@salford.ac.uk (+44) (0)161 - 295 - 6480. INTRODUCTION

E N D
General Anaesthesia and Day-case Patient Anxiety Dr. Mark Mitchell Faculty of Health and Social Care University of Salford Manchester England. m.mitchell@salford.ac.uk (+44) (0)161 - 295 - 6480
INTRODUCTION In the later part of the 20th Century patients remained in a hospital bed during their post-operative recovery period for many days. Patients could also remain in hospital for a number of weeks. Watson (1979) Medical-Surgical Nursing and Related Physiology Saunders, London. As a result of the ensuing patient incapacity, the organisation and delivery of physical aspects of nursing care dominated.
Aspects such as wound dressings, pain management, comfort, hygiene, general and specific pre and post-operative care consumed much nursing time and intervention. Pearce (1975) A General Textbook of Nursing: A Compendium of Nursing Knowledge. Faber and Faber, London. The model of nursing by Roper, Logan & Tierney (1980) with a central focus on the Activities of Daily Living was thereby widely used and highly appropriate. Roper, Logan & Tierney (1980) Elements of Nurs: A model for nursing based on model living. Churchill-Livingston: London. However, as the surgical assault on the body has diminished, the need for many such traditional aspects of physical nursing intervention has also diminished. Suhonen et al (2007) Day-case surgical pts health related quality of life. Int. Jour Nursing Practice. 13(2) 121.
Cutting people open is no longer the focus of modern day surgery. Planned and emergency surgery must be separated. An increase in day surgery is crucial not only for saving money but also patients recovery quicker. "In recent years we have seen the biggest changes to surgical practice since its inception as a medical and scientific discipline in the nineteenth century.” Darzi (2007) Saws & Scalpels to Lasers & Robots - Advances in Surg. London: DoH (p. 6). We are therefore witnessing the greatest changes to elective surgical practice in 200 years.
Once back on the ward, post-operative recovery for the modern surgical patient is now quick and many patients only require limited physical nursing intervention. Kingdon & Newman (2006) Determining pt discharge in an OP surg. Setting. AORNJ. 83(4) 898. Such a transformation in surgical practice is providing the opportunity for a much-needed change in emphasis for peri-operative nursing intervention in modern surgery. Gilmartin (2007) Contemporary DS: Patient experience of discharge and recovery. Jour Clinical Nursing. 16(6) 1117.
A number of studies, spanning many years, have consistently reported much patient anxiety prior to elective day surgery. Mitchell (2007) Nurs. research into DS: A Lit. Review. Amb. Surgery. 13(4) 1. Mottram (2009) Therapeutic rels in ds. Jour Clin Nurs. 18(20) 2830. Many patients have been reported to require an increased level of peri-operative psychological support. Stomberg et al (2008) Clinical pract. & routines for DS in Sweden: improved nurs. interven. Jour PeriAnesth. Practice. 23(5) 311. With the demise of many physical aspects of nursing care, the opportunity in which to provide more formalised care of this nature may be emerging. Tse & So (2008) Nurs. perception peri-op teaching amb. Surg. pts. Jour Adv Nurs. 63(6) 619.
METHODOLOGY Purpose - To investigate adult patient anxiety prior to elective day surgery and general anaesthesia. Aims - • Establish the degree of anxiety arising from elective day surgery and general anaesthesia. • Uncover specific aspects patients find anxiety provoking. • Gain evidence to help establish more formal psychological interventions.
A convenience sample of patients scheduled for elective surgery within three public Day Surgery Units in the United Kingdom were invited to take part in the study. Data were collected over a two year period (2005 - 2007). The study was part of a larger study (n=674) gaining the views of day surgery patients. The questionnaire contained n=59 items and followed the main themes of the whole study, that is, questions concerning the environment, hospital personnel and patient experience of anaesthesia. However, only the aspects relating to the environment and general anaesthesia will be examined here.
RESULTS Participants (n=460) underwent a variety of surgical procedures with Gynaecological surgery, General Surgery and Orthopaedic Surgery being the most frequent. Briefly, some of the main descriptive pre-operative findings – 50% of patients (n=229) desired a detailed level of information provision. Additionally, the majority of patients 87% (n=403) desired this information 1 - 4 weeks in advance.
85% of patients experienced some anxiety prior to surgery and general anaesthesia. Waiting in turn to go to theatre gave rise to much anxiety for 59% (n=270) of patients.
The thought of dying during anaesthesia was anxiety provoking for 48% (n=220) of patients. Additionally, the thought of not waking up from the anaesthetic was anxiety provoking for 48% (n=220) of patients.
The anaesthetist explaining events prior to surgery was calming for 78% (n=357) of patients. Physical contact with the nurse immediately prior to anaesthesia was desired by 48% (n=220) of patients although significantly more females preferred this than males.
Holding the hand of a nurse immediately prior to anaesthesia (n=460) (48%)
All items specifically relating to pre-operative anxiety were also entered into a further statistical test named ‘Factor Analysis’. This test examines associations between variables, based on the correlations between them to uncover any emerging patterns. …..EXAMPLE - Online clothes/ book stores frequently state “people who bought this also bought this”. This is just how factors analysis works. The items and subsequent themes developed were -
Nurse explaining events Anaesthetist visiting Anaesthetist explaining events Told the length of anaesthesia Told when can eat and drink again Told what will happen next Pre-operative Anaesthetic Information
Thought of anaesthetic mask over face Thought of losing all control Though of waking up during surgery Thought of having to trust strangers Thought of dying while sleeping Though of not waking up afterwards Anaesthetic Catastrophising
Waiting to go to theatre Thought of removing false items Thought of arriving at theatre door Imminence of Surgery
The issues associated here with - 1) Pre-operative Anaesthetic Information (anaesthetists’ visit, anaesthetist & nurse explaining) 2) Anaesthetic Catastrophising (waking during surgery, not waking afterwards) 3) Imminence of Surgery (waiting, arriving at theatre door) could explain 30% of the variance in ratings of anxiety on the day of surgery. In more simple terms -
If this Pie chart were to represent the total amount of patient anxiety on the day of surgery 30% of anxiety can be explained by the issues associated here with - Pre-operative AnaestheticInformation Anaesthetic Catastrophising Imminence of Surgery ANXIETY
The issues concerning - Pre-operative Anaesthetic Information Anaesthetic Catastrophising Imminence of Surgery are thereby reasonable predictors of Increased levels of anxiety on the day of surgery
SUMMARY Much patient anxiety was generated under these newly formed headings of - 1) Anaesthetic Information Provision: Need for information/ uncertainty of information. Elements concerning induction of general anaesthesia such as mask over the face, length of anaesthesia and trusting strangers. 2) Anaesthetic Catastrophising: Anxiety regarding intra-operative management such as waking up during surgery, dying while anaesthetised or not waking up afterwards. 3) Imminence of Surgery: Waiting their turn for theatre. Arriving in the theatre, seeing medical equipment.
CLINICAL RECOMENDATIONS 1) Pre-operative Anaesthetic Information 50% of patients desired a detailed level of information provision. This desired level of surgical and anaesthetic information is required 1 - 4 weeks in advance of the day of surgery. Initial provision of such information on the day of surgery was too late for the majority of patients. Integrated Care Pathways have been described as ‘structured, patient-centred maps of care” and inclusion of such aspects of care in this documentation may be of great benefit to future patient management. Fisher & McMillan (2004) Integrated care path. for Day Surgery Patients. Colman: Norwich UK (www.daysurgeryuk.org) Timmins & McCabe (2009) Day Surgery: Contemp. Approach Nurs. Care Wiley-Blackwell: UK.
2) Anaesthetic Catastrophising Misconceptions regarding anaesthesia together with other aspects of information must again be provided 1 - 4 weeks in advance of surgery. Catastrophising thoughts such as waking up during surgery, not waking afterwards or dying under anaesthesia should be explored in advance as they may be common amongst patients awaiting anaesthesia (Payne et al. 2003). RCoA (UK) have stated patient-centred anaesthetic information provision for the effective management of anxiety cannot be underestimated (Lack et al 2003). Lack et al (2003) Raising the Standard: Info. for patients. RCoA and AAGBI, London. Payne et al. (2003) Anaesthesia for day case surg: A survey UK adult practice. European Journal of Anaesthesiology. 20(4), 311.
3) Imminence of Surgery The interpersonal skills of the anaesthetist and nurse can be of great value in limiting anxiety(van der Zee et al. 2002). van der Zee et al (2002) Influence of premed consult and prep. info on anxiety patients for cardiac surg. Anxiety, Stress & Coping. 15(2), 123. Aspects also determined to be of benefit to patients are close physical support, words of encouragement (Kaldenberg & Becker 1999) and methods of distraction (Pearson et al. 2004). Kaldenberg & Becker (1999) Eval. care by amb. surg patients. Health Care Man. Review 24(3), 73. Pearson et al (2004) Best pract DS: Review of evid. Amb. Surg 11(1 - 2), 49.
CONCLUSION The Nursing Profession must naturally always be guided by medical innovation. However, Nursing is also professionally obligated to enhance such innovation and not to be merely instructed by it. The nursing-based knowledge outlined here has the potential to be an effective addition to ongoing surgical and anaesthetic innovation in modern elective surgery. As the use of Integrated Care Pathways continues to grow, nursing knowledge regarding formal anxiety management could be an inclusive aspect. Finally, it is impossible to completely eradicate all patient anxiety during the brief episodes of hospitalisation and limited contact with unfamiliar staff.
However, more taught, planned and deliberate attempts to manage anxiety more effectively must become a central feature of modern surgical nursing and occupy the ground vacated by the now largely redundant physical intervention approach to surgical nursing care. M. Mitchell (2009) General anaesth. & patient anxiety. Jour. Advanced Nursing. Vol.66 No.5 p. 1059 – 1071.