Download
1 / 72
850 likes | 3.74k Views
VESTIBULAR DISORDERS. MAINTAINING BALANCE. Requires the maintenance of COG within the BOS Requires adequate m strength, control, selection of appropriate strategies and the ability to organize sensory input. Age related changes that affect balance. Dec. reaction time

E N D
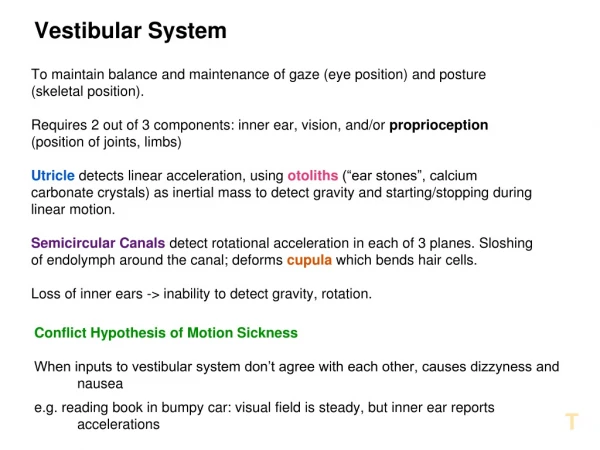
MAINTAINING BALANCE • Requires the maintenance of COG within the BOS • Requires adequate m strength, control, selection of appropriate strategies and the ability to organize sensory input
Age related changes that affect balance • Dec. reaction time • dec. proprioception of the feet • dec. vibratory sense of the toes • inc. sway while standing • significant dec. in vestibular sensory input
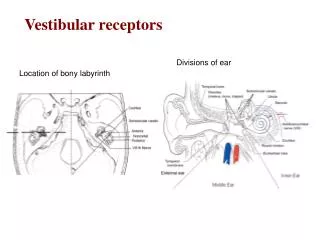
Anatomy and physiology of the peripheral vestibular system • Located in the temporal bone and is made up of three semicircular canals posteriorly, the vestibule in the middle, and the cochlea anteriorly. • Membranes are filled with endolymph
Peripheral vestibular system • Consists of semicircular canals, utricle and saccule, otoliths, and vestibular nerve. • Sensory epithelium lining the utricle and saccule contains hair cells that are embedded in the otolithic membrane, which is gel-like and contains calcium carbonate crystals. • This sensory lining responds to quick tilting mvt. of the head and rapid linear acceleration and deceleration.
Otolith structures • Otolithic membranes cause bending of the hairs in one direction or another. Except when the otolithic membrane is in a horizontal plane. • Detect position of the head with respect to gravity and sense translational movements in which the head is steady but the body as a whole moves.
Saccule • Senses vertical movement as when going up in an elevator
Utricle • Detects horizontal movements such as when one is in a car moving forward
Semicircular canals • Ant. Post. and lateral semicircular canals are at right angles to each other • Detect angular head movement in all planes • Function to generate compensatory eye movement and also to generate postural movements
VOR • Stimulated in response to head movement • Serves to allow one to maintain focus on a target while the head is moving • Causes eye movements that are = in magnitude but opposite in direction of head movements
Pathology of the vestibular system • Categorized as perpheral or central disease. • In acute injury, the firing rate of the vestibular nucleus on the side of the lesion is decreased • Unilateral lesions of the peripheral vestibular system cause disruptions of the vestibulospinal reflexes and the VOR which can be static or dynamic
Pathology con’t • Static disturbances of the VOR causes spontaneous nystagmus because of imbalance of the vestibular nuclei • Impaired vestibulospinal reflexes causes wide based ataxic gait pattern and dec. dynamic postural control • Disruption of the semicircular canals results in vertigo- the world is spinning(or person)
More pathology • Otolith dysfunction causes the pt. to feel as though they are tilting, moving vertically, or ant/posteriorly. • Bilateral vestibular deficits causes severe dynamic disturbance in the VOR and vestibulospinal reflexes. Oscillopsia and significant postural instability
Vestibular disorders • Labyrinthitis and Vestibular Neuritis • comes from inflam. Of inner ear and/or auditory or vestibular nerve because of infection • Sudden onset vertigo, nausea, unilateral hearing loss and tinnitus. Vestibular neuritis no hearing loss • Sx last 12-36 hours resolve over time. May c/o lightheadedness inc. by rapid head mvt.
Benign Paroxysmal Positional Vertigo • (BPPV) caused by head trauma, inner ear infestion, degeneration of inner ear structures • Asymmetrical vestibular response to head mvt. Caused by an inappropriate response in one of the semicircular canals that stimulates fluid flow in the affected canal. Also caused by otolith debris in horizontal canal. • Sx. Position vertigo,dizziness,disorientation
Meniere’s Disease • Etilogy-unknown. Possible pressure imbalance in endolymph • Spontaneous episodes of extreme vertigo, nausea,ear fullness, tinnitus, and unilateral hearing loss • Sx last several hours and may result in disequlibrium • Recurring episodes
Ototoxicity • Exposure to ingestion of a chemical agent or med that is known to damage the auditory or vestibular system. Salicylates, anticonvulsants and some diuretics may reverse. Streptmyocin, neomycin and gentamicin may be permanent • Sx. Vertigo and disequilibrium
Perilymph Fistula • Caused by an abnormal opening between the air space in the middle ear and the fluid filled space in the inner ear that results in leakage of fluid into the middle ear and stimulation of the inner ear organs. • Recent head/ ear injury, infection change in air pressure • Sx. Brief dizziness/vertigo, disequlib., nausea brought on by pressure changes
Central dizziness • Dysfunction at the vestibular nuclei and connections with cerebellum and BS • Sx. Constant feeling of unsteadiness • Poor candidates for vestibular rehab
Idiopathic Vestibular Degeneration • Unknown cause. Seen in the aged. Degeneration of the ear structures • Sx. Multisensory dizziness with impaired vision, proprioception, and vestibular functions, unsteadiness and frequent falls
Acoustic Neuroma • Tumor in the internal auditory canal or cerebellopontine angle • Sx. Gradual unilateral, hearing loss, unilateral tinnitus, mild dizziness, ear pressure, ear fullness. Large tumors affect the facial nerve
Vestibular Migraines • Occur with headaches • Sx short spells of vertigo from 2-20 minutes
Vascular disorders • Vertebrobasilar artery insufficiency, which leads to hypofusion and ischemia of areas within the vestibular system, including the labyrinth and brain stem. • Common cause of vertigo in those over 50 • Sx. Abrupt vertigo, lasting several minutes with nausea and vomiting • Sx. Visual hallucinations, drop attacks or weakness, visual field cuts, diplopia and headaches help to confirm DX.
Otologic Tests • Audiometric evaluation • Tests of VOR system-caloric test, visual autorotation test, and electronystagmography • information about the symmetry of a vestibular lesion affecting the horizontal semicircular canals • useful in determining the appropriate interventions to promote gaze stab. and habituation to dizziness
VOR Testing • Eyes should move at the same speed as the head, with no abnormal latency or delay • The amt. Of eye movement (gain) should be equal to the amount of head mvt. • VOR is tested for: • speed (phase) • strength (gain) • symmetry
Caloric test • Only test that checks the function of one vestibular apparatus at a time
Visual autorotation • Measures the function of the horizontal semicircular canals and the gain and phase patterns for vertical or horizontal VOR • Assymmetry indicates a peripheral lesion, the eyes deviate toward the impaired side
Electronystagmography • Series of tests that assess spontaneous and positional nystagmus • Allow for sensitive and accurate recording of eye movements with the eyes open or closed, in darkness or in a lighted room
Examination • Distinguish between s&s of peripheral and central vestibular lesions in order to implement appropriate interventions • Multisystem involvement may complicate this as in DM, CV disease or arthritis
Patient History • Caregiver may be present for your interview • Of import: Hx of current condition and prior tx received, functional level including any recent declines, medications (ototoxic drugs), other tests and measures, past history of present condition, PMH, PSH etc.
History of current condition • Questions regarding course- onset, duration, and frequency • Precipitating, exacerbating, and relieving factors; and associated symptoms
Symptoms associated with peripheral disease • Peripheral vestibular disease • Distinct episodes and/or sudden onset of sx • Dizziness lasting <1 minute (BPPV) • Dizziness lasting hours with a gradual dec. ( labyrinthitis, neuritis, Meniere’s dis) • Motion provoked disequilibrium • Sx that inc. or occur with change in head position or eyes closed • tinnutis, hearing loss, ear pain, or fullness, esp. if unilateral
Central vestibular disease • Gradual onset • Dizziness lasting >24 hours without decline • Lightheadedness and disequlibrium without motion • Symptoms unaffected by position change • Slurred speech, syncope,near syncope, numbness, tingling of face or extremities, diplopia
Diseases mimicing vestibular disease • Postural hypotension • Sx. Only in standing • Peripheral neuropathy • Bony changes in the spine or vertebral artery disease
Past medical history • Focus on hx of head trauma or rapid pressure change, positional vertigo, ototoxic drug or chemical exposure, food allergies, peripheral neuropathies, noise exposure, autoimmune disorders, psychiatric disorders, surgeries, viral and bacterial infections,significant eye disease, demyelinating disease, epilepsy, PD, brain tumors, CVA, TIA,migraine may indicate a central cause
Functional Status and Activity level • Ask about ADLs, IADLs, • Older persons with vestibular disease or balance disorders may dec. their activity levels to minimize sx. Therefore have dec. strength and ROM
Meds • Recent or current use of antidepressants, sedatives, tranquilizers, and vestibular suppressants(meclizine) can cause cerebellar brain stem sx. Some duiretics may cause transient vestibular hypofunction
Aerobic capacity cognition use of assistive devices community integration cranial nerve integrity barriers integument jt. integrity Mobility motor function sensory integration posture ROM self care/home management sensory integrity static/dynamic postural control Tests and measures
Visuomotor tests • Static exam: • Peripheral disease nystagmus is horizontal or rotary and diminishes with visual fixation • Central disease nystagmus is vertical and may inc. with visual fixation. May also be more intense in one eye • In spontoneous nystagmus, note the direction, ask pt. to fix on a target and see whether the nystagmus changes
Visuomotor tests con’t • Dynamic exam: • Head shaking is used to predict unilateral vestibular disorders • Close eyes , flex to 30, shake as in saying NO for 15 sec with eyes closed. Partially uncompensated vest loss affecting horizontal canals results in nystagmus, beating away from the lesion site
Rotational tests (VOR) • Ask pt. to focus on your finger. While looking at your finger, rotate the head as in NO, first at slow speeds then faster. As speed increases look to see whether visual fixation is maintained or pt. loses visual contact and must make saccades to regain visual contact with the target. • Eval the accuracy and speed of tracking
Oculomotor tests • Used to eval the integrity of cerebellum in producing efficient eye mvts by assessing pts. control of eye mvt. • Saccades are vol or reflexive rapid eye mvts. To bring the target in line with the center of vision • Smooth pursuits are used to maintain stable gaze on objects that are moving within the visual field • Accurate smooth pursuits match the velocity of the target. • Gross abnormalities indicate the need to see a Neurologist
Hallpike Maneuver • Used to elicit nystagmus and vertigo commonly associated with BPPV • Pt is seated, eyes open, head is turned 45 pt is brought rapidly into ext in supine. In BPPV the pt. will have vertigo and rotary nystagmus after 2-15 sec. Symptoms last 15-45 sec. Pt is then brought back up to sitting. Direction and duration are related to which of the semicircular canals are affected
Romberg test • Assess the integrity of vertical semicircular canals, involved with the vestibulospinal pathways for balance control.
Other tests • Orthostatic tests • Limits of stability • Computerized dynamic posturographic studies • CTSIB • POMA • Berg
Interventions for Vestibular Disorders • Meds • meclizine or dimenhydrinate. Acute symptoms • may retard natural vestibular compensation process and limit full recovery of balance function • side effects slowing of mental processing and reaction time
Vestibular Rehabilitation • Uses interventions to eliminate of decrease symptoms associated with peripheral vestibular pathology. • Consists of exercises to promote: • adaptation • substitution • in order to decreases symptoms and maximize balance
Types of exercises • Repeated head mvts. To promote habituation to dizziness • Positioning maneuvers to prevent onset of vertigo • Exercises to improve eye-head coordination,fixation of gaze and balance retraining
Rationale • Designed to incorporate visual and proprioceptive cues because the vestibular system interacts with both of these systems • Simulate conditions that produce symptoms in the environment by using small and full visual field stimuli • Focuses on compensatory strategies for managing safely in the environment, fall prevention LE ROM and strengthening as well as aerobic conditioning
Frequency and duration • Usually 4-8 weeks with PT OT as required for impairments additionally 1-2 per week • Specific home program that is very progressive. These pts may need to do the HEP indefinitely. • Pt participation and compliance is a must