Download
1 / 72
770 likes | 1.38k Views
Vestibular Disorders. Meniere’s Disease Endolymphatic Hydrops Michael J Disher, MD Ear, Nose, and Throat Associates For Wayne, Indiana. Dizziness. Imprecise Term Lightheadedness Imbalance / Unsteadiness Faintness / Giddiness Sensation of Swimming or Floating

E N D
Vestibular Disorders Meniere’s Disease Endolymphatic Hydrops Michael J Disher, MD Ear, Nose, and Throat Associates For Wayne, Indiana
Dizziness Imprecise Term • Lightheadedness • Imbalance / Unsteadiness • Faintness / Giddiness • Sensation of Swimming or Floating • Episodes of Mental Confusion • Minor Seizure
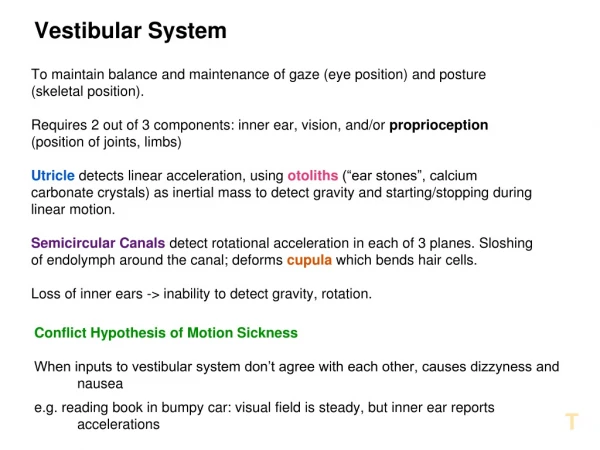
Vertigo Hallucination of Motion • Subjective Vertigo “I’m spinning” • Objective Vertigo “The room is spinning” Does not Localize “Chãng mÆt”
Epidemiology • 11.3 Million Visits per year involve a complaint of dizziness • 5%-10% of all initial visits to MDs • Dizziness ranks 10th by age 65 • Ahead of low back pain and headaches • 40% of population over the age of 40 will experience dizziness • NIH Study
Initial Management • Rule Out Non-Vestibular Causes • Cardiac • Neurologic • Systemic • Not unlike a syncope evaluation
Warning Signs • Cardiac Findings • Neurologic Findings • True Loss of Consciousness • Facial Paralysis • Pain • Headache • Cervical Pain • Otologic Findings • Sudden Hearing Loss • Purulent Drainage • Otalgia
Initial Management • Rule - out Acute Event • Neurologic and Cardiac Evaluation • Control Initial Symptoms • Antivert (Meclizine) • Valium (Diazepam) • Phenergan (Promethazine HC) • Patient Education and Support • Majority of patients with an acute balance disorder recover spontaneously with only symptomatic treatment
Medical Treatment Vestibular Suppressants • Antivert (Meclizine) • Antihistamine • Tablets 12.5mg, 25mg, 50mg • Dose 25mg TID prn • Adverse Reactions • Drowsiness • Rarely • Dry Mouth • Blurred Vision • Caution due to Anticholinergic Effect • Asthma, Glaucoma, Enlarged Prostate
Medical Treatment Vestibular Suppressants • Valium (Diazepam) • Benzodiazepam • Tablets 2mg, 5mg, 10mg • Dose 2mg QID prn • Adverse Reactions • Drowsiness
Medical Treatment Anti-emetics • Phenergan (Promethazine HC) • Phenothiazine • Tablets 12.5mg, 25mg, 50mg • Dose 25mg QID prn • Adverse Reactions • Drowsiness
Compensation • Acute • Cerebellar Clamp • Short term improvement • Significant symptoms remain • Chronic • Central nervous system plasticity • Long-term recovery • Full recovery often possible
Vestibular Compensation • Goals • Gaze Stability • Postural Control • Under both Static and Dynamic Conditions • Characteristics • Enhanced by Head Movement • Delayed by Inactivity • Inhibited by Vestibular Suppressants • Hindered by Preexisting or Concurrent Central Vestibular System Dysfunction • Somewhat Fragile and Energy-dependant Process
Vestibular NeuritisLabyrinthitis Viral Cochleitis • Acute Vestibular Crises • Severe Vertigo 12 - 24 hours • Residual Motion provoked Symptoms for days - weeks • Gradual Improvement • Compensation • Hearing Loss = Labyrinthitis • Stable Uncompensated Lesion
Vestibular Neuritis Labyrinthitis Acute Management • Rule-out Acute Event • Neurologic and Cardiac Evaluation • Vestibular Suppressants • Education and Reassurance
Vestibular Neuritis Labyrinthitis Long-Term Management • Increase Activity • Wean Vestibular Suppressants • Education and Reassurance • Vestibular Exercises • Vestibular Rehabilitation Therapy
Vestibular Rehabilitation Therapy Goals • Reduce symptoms provoked by motion or position • Improve equilibrium • Improve quality of life by increasing activity levels
Vestibular Rehabilitation Therapy What happens in VRT? • Assessment • Find movements and positions which provoke symptoms • Look for stance and gait problems • Assess Risk for falls • Look for other physical problems which might limit VRT • Education and Reassurance • Home Exercise Program (HEP) • Habituation Exercises • Small, controlled, repeated doses of provocative movements • Graduated Program • Balance and Gait Training • General Conditioning
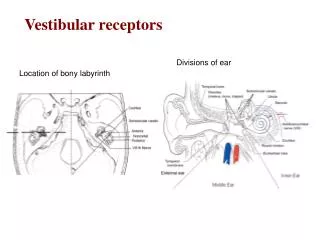
Meniere’s DiseaseEndolymphatic Hydrops CochlearCross-sectional Anatomy
Temporal Bone Cross-sectional Anatomy Mild Hydrops
Temporal Bone Cross-sectional Anatomy Severe Hydrops
Endolymphatic Hydrops(Meniere’s Disease) • Episodic Severe Vertigo Lasting for Hours • Fluctuating Low Frequency Hearing Loss • Roaring Tinnitus • Aural Fullness • Unstable Lesion Symptoms
Endolymphatic Hydrops Medical Management • Sodium Restriction • 1500 - 2000 mg per day • Not just ‘no salt shaker’ • Must change eating habits • 64 oz fresh water per day • No Water Softener, which may add salt • Diuretic • Avoid Caffeine, Sugar, Nutrasweet, Tobacco
Endolymphatic Hydrops Intratympanic Decadron • Advantages • Non-Destructive • Helpful with Hearing Loss • Disadvantages • Less Effective than Gentamicin
Endolymphatic Hydrops Intratympanic Gentamicin • Advantages • 70-90% Control of Vertigo • Office Procedure • Disadvantages • Destructive Procedure • Risk of Hearing Loss
Endolymphatic Hydrops Meniett • Advantages • 50%-70% Control of Vertigo • Non-Destructive • Disadvantages • Requires PET
Endolymphatic Hydrops Surgical Management Endolymphatic Sac Shunt / Decompression
Endolymphatic Hydrops Endolymphatic Sac Shunt / Decompression Surgical View
Endolymphatic Hydrops Surgical Management Endolymphatic Sac Shunt / Decompression
Endolymphatic Hydrops Surgical Management • Endolymphatic Sac Shunt / Decompression • Advantages • Non-Destructive • Hearing Preservation • Out - Patient Surgery • Disadvantages • Controversial • ? 50% - 90% Effective • Surgical Morbidity
Endolymphatic Hydrops Surgical Management Vestibular Nerve Section
Endolymphatic Hydrops Vestibular Nerve Section
Endolymphatic Hydrops Vestibular Nerve Section
Endolymphatic Hydrops Vestibular Nerve Section
Endolymphatic Hydrops Surgical Management • Vestibular Nerve Section • Suboccipital vs.. Middle Cranial Fossa • Advantages • 95% Control of Vertigo • Preserves Hearing • Disadvantages • Intracranial Procedure • Destructive Procedure
Endolymphatic Hydrops Surgical Management Labyrinthectomy
Endolymphatic Hydrops Labyrinthectomy
Endolymphatic Hydrops Surgical Management • Labyrinthectomy • Advantages • 95% Control of Vertigo • Extracranial Procedure • Disadvantages • Destructive Procedure • Sacrifice Hearing
Migraine Headaches • 20,000 Patients Diagnosed with Migraine Who had HA at least once per year • 17.6% Adult females • 5.7 % Adult males • 4% children • 18% had HA one or more per month • Highest prevalence 35-45 years • Lowest prevalence > 50 years • Of those in the 20,000 deserving Dx of Migraine only • 29% males and 41% females aware Prevalence Study
Migraine Events • Migraines are Neurological events • Most common symptoms is Headache • Events can range from no pain to severe pain with permanent ischemic damage • Most common non-pain form of a migraine is visual, but any aura symptom can occur in the absence of pain, including dizziness
Migraine Events HIS Classification • Migraine without aura • Migraine with aura • Migraine with prolonged aura • one Symptom lasts > 60 min but < 7 days • Basilar migraine • Migraine aura without headache • Childhood periodic syndromes • Migrainous infarction
Migraine Head Ache History Clues • Head pain localizes • May be associated with eyes • Throbbing • Light or sound sensitivity - motion sickness especially in childhood • Scintillating lights - with or without pain • Family members with migraine • Mild to severe - hormonal and food triggers • Headache with caffeine withdrawal
Migraine classification - IHS • Migraine without aura (“Common migraine”) • At least five attacks meeting the criteria below • Duration 4-72 hours • Headache has at least two of the following: • Unilateral location • Pulsating quality • Moderate to severe intensity (inhibits or prohibits daily activities) • Aggravation with physical activity that increases intra-cranial pressure, eg. Walking stairs, straining,, etc • During headache at least one of the following: • Nausea and / or vomiting • Photophobia and / or phonophobia