Download
1 / 69
690 likes | 916 Views
Staphylococcal Infection. Bacteriology. Bacteriology. Gm +ve cocci Cluster Facultative Nonfastidious. Classification. Classification. Staph. Aureus; Coagulase positive Staph. Epidermidis; Coagulase negative. Staph. Aureus Infections. Mechanism of pathogenesis;

E N D
Bacteriology • Gm +ve cocci • Cluster • Facultative • Nonfastidious
Classification • Staph. Aureus; Coagulase positive • Staph. Epidermidis; Coagulase negative
Staph. Aureus Infections • Mechanism of pathogenesis; 1-coenzymes local destruction 2-Secretion of Toxins 3-Superantigens activating T cell receptors 4-Interfer with opsonophagocytosis
Epidemiology • Normal human flora; nose& moist areas • Transmission; Hands/nose sec/contact/rarely air. • Colonize; skin, newborn nasoph& umb. • Invasion; Skin breaks, I/V access, immune defect, steroids and neutropenea.
Clinical conditions • Suppurative. • Toxic related;
Clinical conditions • Suppurative. • Toxic related; Scalded Skin Syndrome SSS Toxic Shock Syndrome ??Kawasaki’ Disease Food poisoning
Skin • Foliculitis • Furaculosis (Boils)/Carbunkles • Emptigo contagoesa • Bullous Emptigo • SSS (Ritter disease)
Respiratory Infections • Sinusitis • Parotitis • Cervical adenitis • Tracheitis compared to croup • Pnumonia;
Sepsis • Start as focal lesion e.g. a boil • Yield to septicemia • Localize to organs e.g. lung, bone, heart, brain etc
Muscles/Bone/Joints • Tropical pyomyositis; Localized abscesses and high CPK • Osteomylitis; Trauma/Sx, pain, fever • Septic arthritis; Usually hematogenous
CNS • Meningitis; Bacteremea, O.M, skull osteo., neural canal defects. • Neurosurgical procedures and VP shunt
Heart • Bacterial endocarditis; -Perforated heart valve -myocardial abscess -purulent pericarditis -Sudden death
Kidney • Perinephric abscess • UTI; Staph. saprophyticus (CONS) Sexually active adolescent girls
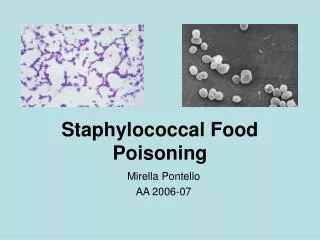
G.I. • Food poisoning; Meat, mayonnase, creamed foods Short incubation period of 1 to 7 HRs Perfuse vomiting, no fever Test susp. food for staph bacteria/ toxins
Diagnosis • Isolate staph. bacteria • Gram stain • Identify Toxins
Treatment • Penicillinase resistant antibiotics; Oxacillin (Cloxacillin, Flucloxacillin) methicillin Nafcillin 1st generation cephalosporine, cefazolin (Ultracef)
Treatment cont. • Betalacamase hyperprodcer staph.; Amoxicillin/Clavulenic acid(Augumentin) Ampicillin/Salbactam Imipenem Fluoroquinilones 1st generation cephalosporin Vancomycin
Coagulase negative Staph. (CONS) • Common Skin Flora • Ubiquitous organism • Has affinity to plastic (surface hydophobicity & production of slim) • Neonates, I/V access and shunt devices infections (nosocomial infections)
Clinical Conditions • Premature neonatal sepsis/NEC. • Older children sepsis is rare (minimal signs of sepsis) • Persistent pactreamia usual with indwelling devices (I/V cath, VP shunt, cardiac grafts and prosthesis etc.)
Clinical Cond. Cont. • Single positive blood culture is a contaminant • UTI in adolescent girls Staphylococcus Saprophyticus (CONS)
Treatment • Remove the access devices/shunts. • May externalize the VP shunt. • Vancomycin or Rifampin. • Amoxicillin or Quinolones for the Staph Saprophyticus UTI.
Definition Infections not present or incubating at the time of admission that develop during admission or less than one incubation period after discharge
Definition cont. Infections 48 HRs or more after admission is assumed to be nosocomial unless the infection is clearly community acquired
Clean Surgery Incision through prepared normal skin and the operative field dose not include infected tissue , abscess, or entry into normally unsterile areas such as the bowel, the upper respiratory tract, or the lower female genital tract.
Rate of Nosocomial Infections Number of nosocomial infections divided by the number of patients at risk multiplied by 100
Epidemiology • 1/3 hospital infections are nosocomial (estimate in the USA) i.e. 2 million patients i.e. 4 million patient days of hospitalization i.e. 4.5 Billion USD i.e. 17 Billion SAR
Epidemiology cont. In USA (1978) nosocomial inf. rate; -All services 3.37% -Pediatric services 1.2%