Download
1 / 49
490 likes | 902 Views
Bronchopulmonary Dysplasia(BPD). Kumari Weeratunge M.D. PL - 2. Back ground. Develops in neonates treated with O2 & PPV . Originally described by Northway in 1967 using clinical , radiographic & histologic criteria .

E N D
Bronchopulmonary Dysplasia(BPD) Kumari Weeratunge M.D. PL - 2
Back ground • Develops in neonates treated with O2 & PPV . • Originally described by Northway in 1967 using clinical , radiographic & histologic criteria . • Bancalari refined definition using ventilation criteria , O2 requirement @ 28days to keep PaO2>50mmhg & abnormalities in chest x –ray .
Back ground • Shennan proposed in 1988 criteria of O2 requirement @ 36 weeks corrected GA . • Antenatal steroids , early surfactant Rx & gentle modes of ventilation minimize severity of lung injury .
Pathophysiology • Multifactorial • Major organ systems - lungs & heart • Alveolar stage of lung development - 36wks GA to 18 months post conception • Mechanical ventilation & O2 interferes with alveolar & pulmonary vascular development in preterm mammals . • Severe BPD Pulmonary HT & abnormal pulmonary vascular development .
Stages of BPD • Defined by Northway in 1967 • Stage 1 - similar to uncomplicated RDS • Stage 2 - pulmonary parenchymal opacities with bubbly appearance of lungs • Stage 3 & 4 – areas of atelectasis , hyperinflation & fibrous sheaths • Recently CT & MRI of chest – reveals more details of lung injury
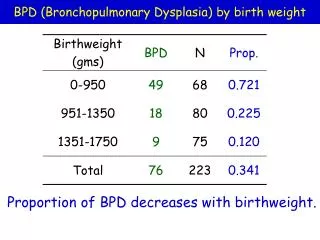
Frequency of BPD • Dependent on definition used in NICU . • Using criteria of O2 requirement @ 28 days frequency range from 17% - 57% . • Survival of VLBW infants improved with surfactant Actual prevalence of BPD has increased .
Mortality/Morbidity of BPD • Infants with severe BPDIncreased risk of pulmonary morbidity & mortality within the first 2 years of life .
Pulmonary Complications of BPD • Increased resistance & airway reactivity evident in early stages of BPD along with increased FRC . • Severe BPD Significant airway obstruction with expiratory flow limitations & further increased FRC secondary to air trapping & hyperinflation
Volume trauma & Barotrauma • Rx of RDS – surfactant replacement , O2 , CPAP & mechanical ventilation . • Increased PPV required to recruit all alveoli to Px atelectasis in immature lungsLung injuryInflammatory cascade . • Trauma secondary to PPV-Barotrauma • VolumetraumaLung injury secondary to excess TV from increased PPV .
Volume trauma & Barotrauma • Severity of lung immaturity & effects of surfactant deficiency determines PPV . • Severe lung immaturityAlveolar number is reducedincreased PP transmitted to distal bronchioles . • Surfactant deficiencysome alveoli collapse while others hyper inflate .
Volume trauma & Barotrauma • Increased PPV to recruit all alveoliCompliant alveoli & terminal bronchioles ruptureleaks air in to interstiumPIEIncrease risk of BPD • Using SIMV compared to IMV in infants <1000g showed less BPD .
O2 & Antioxidants • O2 accept electrons in it’s outer ringForm O2 free radicalsCell membrane destruction • Antioxidants(AO)Antagonise O2 free radicals • Neonates-Relatively AO deficient • Major antioxidants – super oxide dismutase , glutathione peroxidase & catalase
O2 & Antioxidants • Antioxidant enzyme level increase during last trimester . • Preterm birthIncreased risk of exposure to O2 free radicals
Inflammation • Activation of inflammatory mediatorsIn acute lung injury • Activation of leukocytes by O2 free radicals , barotrauma & infectionDestruction & abnormal lung repairAcute lung injuryBPD • Leukocytes & lipid byproducts of cell membrane destructionActivate inflammatory cascade
Inflammation • Lipoxigenase & cyclooxigenase pathways are involved in the inflammatory cascade • Inflammatory mediators are recovered in tracheal aspirate of newly ventilated preterm who later develops BPD • Metabolites of mediatorsvasodilatationincreased capillary permeabilityalbumin leakage & inhibition of surfactant functionrisk of barotrauma
Inflammation • Neutrophils – release collegenase & elastasedestroy lung tissue • Hydroxyproline & elastin recovered in urine of preterms who develops BPD • Di2ethylhexylphthalate(DEHP) degradation product of used ET tubeslung injury • A study in 1996 found that increased interleukin 6 in umbilical cord plasma
Infection • Maternal cervical colonization/ preterm neonatal tracheal colonization of U.urealyticum associated with high risk of BPD
Nutrition • Inadequate nutrition supplementation of preterm compound the damage by barotrauma , inflammatory cascade activation & deficient AO stores • Acute stage of CLDincreased energy expenditure • New born ratsnutritionally depriveddecreased lung weight
Nutrition • Cu , Zn , Mn deficiencypredispose to lung injury • Vit A & E prevent lipid peroxidation & maintain cell integrity • Extreme prematurity – large amounts of H2O needed to compensate loss from thin skin
Nutrition • Increased fluid administration increased risk of development of PDA & pulmonary edema(PE) • High vent settings & high O2 needed to Rx PDA & PE • Early PDA Rx – improve pulmonary function but no effect on incidence of BPD
Genetics • Strong family history of asthma & atopy increase risk of development & severity of BPD
CVS Changes • Endothelial cell proliferation • Smooth muscle cell hypertrophy • Vascular obliteration • Serial EKG – right ventricular hypertrophy • Echocardiogram – abnormal right ventricular systolic function & left ventricular hypertrophy
CVS Changes • Persistent right ventricular hypertrophy/ fixed pulmonary hypertension unresponsive to supplemental O2 leads to poor prognosis
Airway • Trachea & main stem bronchi - abnormalities depend on duration & frequency of intubation & ventilation • Diffuse or focal mucosal edema , necrosis/ulceration occur • Earliest changes from light microscopyloss of cilia in columnar epithelium , dysplasia/necrosis of the cells
Airway • Neutrophils , lymphocyte infiltrate & goblet cell hyperplasiaincreased mucus production • Granulation tissue & upper airway scarring from deep suctioning & repeated ET intubation results in laryngotracheomalacia , subglottic stenosis & vocal cord paralysis
Airway • Necrotizing bronchiolitis – results from edema , inflammatory exudate & necrosis of epithelial cells . • Inflammatory cells , exudates & cellular debris obstruct terminal airways • Activation & proliferation of fibroblastsperibronchial fibrosis & obliterative fibroproliferative bronchiolitis
Radiologic Findings • Decreased lung volumes • Areas of atelectasis • Hyperinflation • Lung haziness • PIE
Histologic Findings • In 1996 Cherukupalli & colleagues described 4 pathologic stages • Acute lung injury • Exudative bronchiolitis • Proliferative bronchiolitis • Obliterative fibroproliferative bronchiolitis
Medical care in BPD • Prevention • Mechanical ventilation • O2 therapy • Nutritional support • Medications
Mechanical Ventilation • O2 & PPV life saving • Aggressive weaning to NCPAP eliminate need of PPV • Intubation primarily for surfactant therapy & quickly extubation to NCPAP decrease need for prolong PPV • If infant needs O2 & PPV gentle modes of ventilation employed to maintain pH 7.28 – 7.40 , pCo2 45 – 65 , pO2 50- 70
Mechanical Ventilation • Pulse oximetry & transcutaneous Co2 mesurements – provide information of oxygenation & ventilation with minimal patient discomfort • SIMV – provide information on TV & minute volumes which minimize O2 toxicity & barotrauma/volumetrauma • SIMV – allow infant to set own IT & rate
Mechanical Ventilation • When weaning from vent & O2 difficult – when adequate TV & low FiO2 achievedtrial of extubation & NCPAP • Commonly extubation failuresecondary to atrophy & fatigue of respiratory muscles • Optimization of nutrition & diuretics – contribute to successful weaning from vent • Meticulous nursing care – essential to ensure airway patency & facilitate extubation
O2 Therapy • Chronic hypoxia & airway remodelingpulmonary HT & cor pulmanale • O2stimulate production of NOsmooth muscle relaxationvasodilatation
O2 Therapy • Repeated desats secondary to hypoxia results from- decreased respiratory drive - altered pulmonary mechanics - excessive stimulation - bronchospasm • Hyperoxiaworsen BPD as preterms have a relative deficiency of AO
O2 Therapy • O2 requirement increase during stressful procedures & feedingstherefore wean O2 slowly • Keep sats 88% - 92% • High altitudesmay require O2 many months • PRBC transfusionincrease O2 carrying capacity in anemic(hct<30%) preterms
O2 Therapy • Study in 1988 found increased O2 content & systemic O2 transport , decreased O2 consumption & requirement after blood Tx • Need for multiple Tx & donor exposures decreased byerythropoetin , iron supplements & decreased phlebotomy requirements
Nutritional Support • Infant with BPD- increased energy requirements • Early TPN – compensate for catabolic state of preterm • Avoid excessive non N calories increase CO2 & complicate weaning • Early insertion of central linesmaximize calories in TPN
Nutritional Support • Rapid & early administration of increased lipidsworsen hyperbillirubinemia & BPD through billirubin displacement from albumin & pulmonary vascular lipid deposition respectively . • Excessive glucose loadincrease O2 consumption , respiratory drive & glucoseuria.
Nutritional Support • Cu , Mn , & Zn essential cofactors in AO defenses • Early initiation of small enteral feeds with EBM , slow & steady increase in volumefacilitate tolerance of feeds • Needs 120 – 150 Kcal/kg/day to gain weight
Medical Therapy • Diuretics • Systemic bronchodilators
Diuretics • Furesemide (Lasix) Rx of choice • Decrease PIE & pulmonary vascular resistance • Facilitate weaning from PPV , O2 /both • Adverse effects – hyponatremia , hypokalemia , hypercalciuria , cholelithiasis , nephrocalcinosis & ototoxicity
Diuretics • Careful parenteral & enteral supplements compensate adverse effects • Thiazide & spiranolactone for long term Rx
Systemic Bronchodilators • Methylxanthines – increase respiratory drive , decrease apnea , improve diaphragmatic contractility • Smooth muscle relaxation – decrease pulmonary vascular resistance & increase lung compliance • Exhibit diuretic effects
Systemic Bronchodilators • Theophyline – metabolized primarily to caffeine in liver • Adverse effects – increase heart rate , GER , agitation & seizures
Prognosis • Pulmonary function slowly improves secondary to continued lung & airway growth & healing • Northway- Airway hyperactivity , abnormal pulmonary functions , hyperinflation in chest x ray persists in to adult hood • A study in 1990 found gradual decrease in symptom frequency in children 6 – 9 yrs