Download
1 / 50
580 likes | 1.65k Views
Hypoxic Ischemic Encephalopathy (HIE) Case Studies. Lisa Jorgenson, MSN, NNP-BC Angela Riley, MSN, NNP-BC Avera McKennan Hospital NICU. Objectives. Review incidence, timing, risk factors, and pathophysiology for HIE Review Sarnet Staging for Encephalopathy Briefly review Whole Body Cooling

E N D
Hypoxic Ischemic Encephalopathy (HIE) Case Studies Lisa Jorgenson, MSN, NNP-BC Angela Riley, MSN, NNP-BC Avera McKennan Hospital NICU
Objectives • Review incidence, timing, risk factors, and pathophysiology for HIE • Review Sarnet Staging for Encephalopathy • Briefly review Whole Body Cooling • Discuss HIE case studies
Definition of HIE • Hypoxic= not enough oxygen to the tissues • Ischemic= a restriction in blood supply to tissues, causing a shortage of oxygen and glucose needed for cellular metabolism (to keep tissues alive) • Encephalopathy= disturbed neurological function
Hypoxic Ischemic Encephalopathy (HIE) • Incidence • Affects 2-3/1000 full term live births, • With annual birth rate of 4 million it is expected 8000-12,000 will be diagnosed with this disorder each year in the USA. • The SD birth rate in 2013 was 11,894 so that would be about 24-36 babies each year in SD. • Accounts for 15-25% neonatal mortality • Accounts for 15-28% of children with cerebral palsy and 25% of all cases of developmental delay
HIE – Timing • Timing of insult occurrence • Antepartum: 20% • Intrapartum: 30% • Antepartum-intrapartum: 35% • Postpartum: 10%
HIE - Etiology • Antepartum • Socioeconomic status (SES) • Maternal thyroid disease • Fetal Growth Restriction • Post-dates • Faulty placental gas exchange • Diabetes • Preeclampsia or severe PIH • Acute • Acute hypotension • Placental separation with uterine hemorrhage
HIE - Etiology • Intrapartum risk factors • Cord strangulation (i.e. Nuchal Cord, Knot in Cord, Prolapsed Cord) • Placental problems • Difficult delivery • Maternal fever • Persistent occiput posterior (OP) fetal position • Uterine abruption or rupture • Abnormal fetal heart rate pattern • Fresh meconium
HIE Pathophysiology • Impaired cerebral blood flow is the principal pathogenetic mechanism underlying neuropathology of hypoxia-ischemia • Brain injury occurs in phases • Acute – During the initial insult • Recovery-After restoration of circulation (reperfusion injury) • Infant evolves from primary energy failure→ reperfusion period→latent phase→secondary energy failure
Primary Energy Failure • Initial increased cerebral vasodilation (secondary to hypercapnia and hypoxemia) • Loss of cerebral autoregulation • Redistribution of organ blood flow • ↑CBF is quickly followed by impairment (bradycardia and hypotension) • Activation of cell death • Neuronal death vs. necrosis • Cell lysis • Excitotoxins • Calcium entry • ↓ATP & PCr • ↑ anaerobic glycolysis • Occurs in the first 30 minutes after insult
Reperfusion Period • Return of CBF • Normal BP and pH • Transient improvement in cytotoxic edema • Absence of seizures (EEG depressed) • Rapidly transitions into the latent phase
Latent Phase of Cerebral Injury • Occurs during hours 6 – 15. • Recovery of oxidative metabolism • Apoptotic cascade (ATP and PCr again ↓) • Secondary inflammation • Receptor hyperactivity • Unlike primary phase, intracellular pH and cardiorespiratory status are usually stable
Secondary Phase of Cellular Injury • Occurs from 3 – 10 days • Failing oxidative metabolism • Seizures (↑ CBF) • Cytotoxic edema • Excitotoxins • Final cell death
Sarnat Stage for HIE • Sarnat Stage 1 (mild encephalopathy) • Hyper alertness • Normal muscle tone, active suck, strong Moro reflex, normal/strong grasp, normal doll’s-eye reflex • Increased tendon reflexes • Myoclonus present • Hyper-responsiveness to stimulation • Tachycardia possible • Dilation of pupils, reactive • No convulsions (unless by other cause, i.e. hypoglycemia) • EEG within normal limits • Usually lasts <24 hours
Sarnat Stage for HIE • Sarnat Stage 2 (moderate encephalopathy) • Hypotonia and lethargy • Increased tendon reflexes • Diminished brainstem reflexes - weak suck or gag, incomplete Moro reflex, sluggish pupil reaction, varying respiration • Possible clinical seizures • At this stage, the condition will either improve & the infant will get better or it will worsen & the infant will deteriorate • Results in ~40-70% death or disability with more cases of disability than death (cerebral palsy, cognitive deficits and seizures)
Sarnat Stage for HIE • Sarnat Stage 2 (moderate encephalopathy) • Recovery • No further seizure activity • EEG returns to normal • Transient jitteriness • Improvement in level of consciousness
Sarnat Stage for HIE • Sarnat Stage 3 (severe encephalopathy) • Clinical Features • Apnea/bradycardia • Mechanical ventilation required to sustain life • Level of consciousness deteriorates from obtunded to stuporous or coma • Seizures within the first 12 postnatal hours, usually multifocal clonic seizures; all display subtle seizures • Severe hypotonia & flaccidity; reflexes depressed or absent • Pupils often unequal; variable reactivity & poor light reflex
Sarnat Stage for HIE • Sarnat Stage 3 (severe encephalopathy) • Deterioration • Occurs within 24 to 72 hours • Severely affected infants often worsen, sinking into deep stupor or coma • Death may ensue • Survivors • Often improve in the next several days to months • Feeding difficulties often develop • Generalized hypotonia is common; hypertonia is uncommon • Almost always result in death or disability with death > disability
HIE - Outcomes • Factors associated with poor outcome: • Apgar score • If score is 0-3 for 20 minutes or more, approximately 60% die • If score is less than 3 at 1 minute & less than 5 at 5 minutes, with abnormal neurologic signs • About 20% die • About 40% are normal • About 40% suffer neurologic sequelae • Encephalopathy • Mild: No subsequent deficits • Severe: 75% die; 25% have sequelae • Disappearance of abnormal neurologic signs by 1 to 2 weeks: good chance of being normal
HIE - Outcomes • Seizures early and/or difficult to control associated with poorer prognosis • Hyperactivity & attention difficulties seen in infants with less severe encephalopathy • Rapid initial improvement indicative of better outcomes • Long-term sequelae based on • Site • Extent of cerebral injury • Duration of abnormal clinical presentation
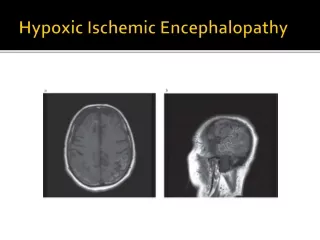
Neuroimaging in HIE • MRI is the primary and most sensitive method for brain injury patterns, timing of injury, and diagnosis of HIE. • Injury to basal ganglia and thalamus is most strongly associated with poorest outcomes.
Mechanism of Action forHypothermia Therapy • Better maintenance of the cerebral energy state • Attenuation of the release of exicitatory neurotransmitters • Decreased caspase -3 activation and morphologic evidence of apoptosis • Reduction in oxygen free radicals • Blockage of inflammatory mediators and inhibition of apoptotic pathways
Whole Body Cooling • Actively works by cooling the head and body together by a water blanket composed of coils • Maintain an esophageal and skin temperature of 32.5°C – 34.5°C
Outcomes in Hypothermia Therapy • Severe HIE – outcomes remain bleak despite cooling • One in 6 babies will garner some benefit • Studies have shown decrease in mortality from 39 -25% and reducing occurrence of cognitive impairments from 28 - 11% • More effective in milder encephalopathy • Either whole body cooling or selective head cooling protocols may be adopted to cool infants with HIE
Avera Childrens’ Hypothermia Program • Established November 2010 • Infants undergo whole body cooling utilizing Blanketrol III system • Undergo 72 hours of active cooling with close monitoring of lab studies and esophageal temperature • Evaluation and follow up with pediatric neurologist and developmental follow up group
Therapeutic Hypothermia – Inclusion Criteria • Before 6 hours of age (mandatory) • ≥35 weeks gestation (mandatory) • History of an acute perinatal event • Apgar score ≤ 5 at 10 minutes • Cord pH ≤ 7.0 or first postnatal blood gas pH ≤ 7.0 within 1 hour • Base deficit on cord gas ≥ 16 mEq/L or first postnatal blood gas ≥16 mEq/L within 1 hour • Continued need for ventilation initiated at birth and continued for at least 10 minutes
Therapeutic Hypothermia – Inclusion Criteria • The attending physician or designee will perform a neurologic exam for infants who did not receive a ABG within one hour of delivery and does not have seizure activity. The infant must show signs of moderate or severe HIE in at least 3 of the 6 categories to be eligible for Therapeutic Hypothermia. • Infants who present with clinical seizures and meet the requirement of an acute perinatal event or have seizure activity with a qualifying blood gas will qualify for therapeutic hypothermia.
Therapeutic Hypothermia – Exclusion Criteria • Inability to enroll within 6 hours • Gestational age <35 weeks • Presence of known chromosomal anomaly • Presence of major congenital anomalies • Severe intrauterine growth restriction (weight ≤ 1800g) • Infants in extremis; no additional intensive therapy planned
Case Study #1 • Risk Factors: variable and prolonged decels, category 2 FHTs, induction at 40.6 weeks for post dates, meconium • Apgars 1 (for present HR) and 8 (-1 color and -1 tone) • Baby born with meconium stained fluid with no tone/resp effort, brought to warmer and immediately intubated for meconium. No meconium noted below cords. PPV initiated and baby improved so changed to CPAP. Blowby continued until 7 mins of age for sats. • Brought to NICU for further care
Initial Lab Results • Cord blood gas: 7.26/40/24/18/-9 arterial and 7.30/35/26/17/-9 venous • Started on oxygen at 2 hours of age for desats. Blood gas 7.37/39/53/23/-2 on NC 1L 30%
NO No NO
Case Study #1 • At 7 hours of age, baby presented with seizure activity. He was loaded with phenobarbital. EEG showed several persistent subclinical seizures that would last up to 5 min. with short interval resolution between episodes. • Baby then loaded with Keppra. Seizures persisted so baby started on a versed drip. Intubated for his heavy sedation/seizure management.
Healthcare Maintenance • Infection: Amp/Gent x 48 hour rule out, Acyclovir, BC negative, LP negative • Neurologic: • CT was essentially normal, no acute intracranial process • MRI- extensive cortical and subcortical signal hyperintensity and diffusion restriction in the left cerebral hemisphere, etiology uncertain. • PedsNeurologist consulted/following patient
Healthcare Maintenance • Fluids, Electrolytes, Nutrition: Initially presented with hypoglycemia and was placed NPO. Started on gavage feedings at 3 days of life. Started feeding by mouth by 7 days of life and feeding ad lib by 11 days of life. • Respiratory: Extubated at 4 days of life. Attempts made to wean NC but still required it for discharge. • Discharge: Home at 14 days of age and 43 weeks gestation
Case #2 • Risk Factors: decreased fetal movement for prior 24 hours, fetal heart tones nonreactive, occasional late decelerations during induction, vacuum assisted delivery • Apgars: 1(heart rate noted),4(2-HR, 1-RR, 1-color),5(2-HR, 1-tone, 1-reflex, 1-color), 6(2-HR, 1-RR, 1-tone, 1-reflex, 1-color) • Baby gave initial gasp, followed by no respiratory effort, infant noted to poor tone and very pale in color
Case #2 • Baby was given PPV with good HR response but still minimal respiratory effort noted, so was electively intubated • No spontaneous movement noted until around 9 min. of age when she opened her eyes • Baby brought to NICU for further care
Initial lab results • Cord arterial gas: 7.17/49/35/17/-10 • Cord venous gas: 7.17/75/39/18/-12 • Capillary gas upon immediate admission to NICU: 6.81/72/42/11.4/-23 • Follow-up arterial blood gas: 7.14/13.5/70/4.7/-24 • WBC-37.7, Hgb-3.2, Hct-11.4, Plt-142, Segs-30, Bands-19
Healthcare Maintenance • Neurologic: Baby was electively cooled per policy • EEG obtained showing no seizure activity • MRI obtained after rewarming DOL 4 showing acute focal infarct on the right with no mass effect or associated hemorrhage • Hematologic: She received 3 rounds of PRBC that day • Respiratory: Extubated by 2 days of life. ENT consult done on day 5 of life for stridor and noted moderate bilateral vocal cord paresis • FEN: Gavage feeds started on day 6 of life and baby began orally feeding by day 10 of life • Discharge: home after spending 17 days in the NICU eating all feeds and thriving
Case Study #3 • 3.5 kg 39 5/7 weeks CGA, G3 P23, vag delivery, nuchal cord x2, meconium stained fluid • Delivery: no respiratory effort, no heart rate, and pale so PPV and chest compressions required. Electively intubated with slow improvement. • Initial blood gas pH 6.9, pCO2 90, HCO3 -15
Healthcare Maintenance • Neurologic: Whole body cooling initiated per protocol • EEG was normal • Head US normal • MRI showed left periatrial white matter ischemic changes • Respiratory: Severe pulmonary hypertension, intubated x 16 days, HFOV x 7 days • Cardiovascular: PPHN, hypotension upon rewarming requiring dopamine and dobutamine along with hydrocortisone
Healthcare Maintenance • Infectious: Amp/Gent x 5 days for clinical sepsis and Acyclovir x 48 hours until HSV culture came back negative • Hematologic: Developed DIC, thrombocytopenia, anemia • Renal: mild renal failure with decreased urine output • Discharged at 33 days and 44 3/7 weeks feeding ad lib on demand
Case study #4 • Risk factors: Unplanned pregnancy with no prenatal care, mother admitted to drinking alcohol, delivered at home, • Apgars: Unable to obtain due to delivery at home without medical supervision. • It was noted that infant was delivered into the toilet and had a loose nuchal cord. Nearby person delivered a finger sweep and gave two rescue breaths prior to calling EMS. • He was delivered resuscitation in the ambulance back to the hospital.
Initial lab results • Venous gas at 0920: 7.05/32.5/134/8.8/-20.6 • Extubated to NC and received NS bolus • Follow up gas upon arrival of transport team: 7.14/62/36/22/-7 • WBC 16.9, Hgb 19.7, Hct 56.5, plt 135,000, segs 36, bands 24
Healthcare Maintenance • Neurologic: Baby was electively cooled per policy • Baby was noted to have seizure-like activity - lip smacking, apnea, intermittent tonic posturing of UE>LE, lateral eye deviation, periodic breathing so baby was loaded with phenobarbital • Skull x-ray, Head US and MRI all obtained with all reported within normal limits • Cardiac: Pulmonary hypertension suspected and started on INO 20ppm with good response noted upon initiation
Healthcare Maintenance • Infectious: Treated for with ampicillin/claforan until a positive culture was reported from outlying facility as coag neg staph. Antibiotics were switched to vancomycin and a blood culture was redrawn. Antibiotics were stopped after repeat culture was negative. • FEN: Baby was kept NPO initially with IV fluids of 60ml/kg/day. Gavage feeds started on DOL 5, began oral feeds on DOL 7 and ad lib by 10 days • Discharged home on DOL 12
Avera McKennan’sSummary of TBC infants • Total of 14 patients have received total body cooling since the start in 2011 • 5 Had EEG confirmed seizures • 6 were placed on anti-seizure medications • MRI findings- 4 Showed evidence of HIE • 7 had no signs of HIE • Neurologic assessment upon discharge • 8 had normal exams • 4 had abnormal exams • ***2 infants were electively taken off life support, given the grim outcome**
References • Department of Health, NSW. Whole Body Cooling – Neonates-Suspected Moderate or Severe Hypoxic Ischaemic Encephalopathy. Policy Directive, 28-July 2009. • Fatemi, A., Wilson, M., and Johnston, M. Hypoxic-Ischemic encephalopathy in the term infant. Clinics in Perinatology, 2009; 36: 835-858. • Rajadurai, VS. Therapeutic hypothermia for neonatal hypoxic-ischaemic encephalopathy. Annals Academy of Medicine. 2006; v35, 1: 3-5. • Sahni, R., and Sanocka, U. Hypothermia for hypoxic-ischemic encephalopathy. Clinics in Perinatology; 2008; 35: 717-734. • Schulzke, S., Rao, S., and Patole, SK. A systematic review of cooling for neuroprotection in neonates with hypoxic ischemic encephalopathy-are we there yet? BMC Pediatrics. 2007; 1-10. • Wachtel, E., and Hendricks-Munoz, K. Current Management of the Infant Who presents with Neonatal Encephalopathy. Current Problems in Pediatric Adolescent Health Care. 2011; 41: 132-153.