Download
1 / 17
190 likes | 923 Views
Pulse oximetry in general practice By Søren Brorson, MD, GP. Introduction to pulse oximetry. Introduced in the early 1980s Measures the percentage of haemoglobin which is saturated with oxygen (SaO2)

E N D
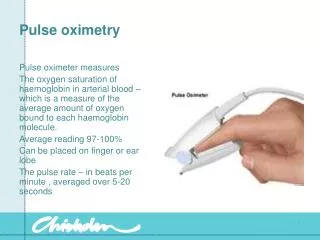
Introduction to pulse oximetry • Introduced in the early 1980s • Measures the percentage of haemoglobin which is saturated with oxygen (SaO2) • Non-invasive, simple, valid, low-cost method of monitoring the oxygen saturation of patients blood • Detect hypoxia before the patient becomes clinically cyanosed (SaO2<80%) • The pulse oximeter is a vital tool in secondary care • A routine vital sign in the emergency medicine • Provides continuous monitoring of oxygenation in anaesthesiology, critical care and transport • Viability of limbs after surgery e.g. vascular grafting • Overnight sleep studies e.g. obstructive sleep apnoea • Exercise testing e.g. shuttle walk test
How does an oximeter work • Consist of a probe which is attached to the patient’s finger and a computerized unit with a display showing SaO2 and pulse rate • Possesses two light-emitting diodes (LEDs), one red and one infrared, and a detector, which derives the oxygen saturation from the intensity of transmitted light during a pulse beat • Plethysmographic waveform display which are useful in assessing the quality of the signal and the effects of artefact • Calibrated during manufacture and automatically check their internal circuits when switched on
Limitations of pulse oximetry • The full picture is not provided, only SaO2 • Arterial CO2 can rise to dangerous levels with still acceptable oxygen saturations • It does not replace clinical judgement • The gold standard for SaO2 is arterial blood gas analysis (PaO2, PaCO2, acid-base balance), but is invasive, painful, time consuming and costly • Pulse oximeters are most accurate at saturations of 70-99% (+/- 2%)
CASE 1 • 45 year-old man brought in to emergency department • Unconscious for 10 min. during BBQ in the patio where he had set up the grill • Physician finds normal cognitiv function, normal neurology, BT 130/80, normal EKG, SAT 97% • Diagnose?
Limitations of pulse oximetry • Pulse oximetry cannot distinguish between different forms of haemoglobins e.g. methaemoglobin and carboxyhaemoglobin absorb light at similar wavelength • Other sources of error lead to signal losses og under-/overestimations of oxygen saturation • Reduced perfusion e.g. cold, cardiac failure • Nail vanish and paint • Ambient light e.g. bright overhead lights • Not SKUB-tested
Does pulse oximetry influence the patient managment ? • Mower ét al. Chest 1995 • Physicians were significantly more likely to change the medical treatment of patients with SaO2<95% compared with patients with SaO2>95% • The oximetry results altered management because the physicians failed to recognize underlying cardiopulmonary difficulties or because they did not realize the severity of the illness • Anderson ét al. Ped Emerg Care 1991 • SaO2 measurements changed the previously assessed degree of illness in 53% of the patients • 13% were deemed more ill and 37% less ill than at the initial assessment • 17% had their management plan changed, 8% were treated more aggressively and 11% less aggressively
CASE 2 • 5 year-old boy, no history of astma or atopi • 2 days with coughing and difficulty in breathing, no fever • A little pale, quiet, tachypnoea, use of accessoric muscles, CRP<10, puls 90, St.p.: rhonchi bilat. SaO2 86% • O2 10 L/min, Ventoline inhalations. SaO2 rises to 96%. Admited to hospital. • CXR: Pneumonia dxt.
Recognition of hypoxia • Respiratory rate is not a reliable screen for hypoxia and is not closely correlated with pulse oximetry measurements • Studies shows that observers have difficulty detecting hypoxaemia undtil SaO2<80% • In one study the pulse oximeter measured SaO2 in 50 pt.’s in A&E. The oximeter identified 21 pt.’s (42%) with clinically unsuspected hypoxia Pulse oximeters in GP may have a role in recognizing hypoxia which otherwise may go undetected - leading to a difference in managment
Recognition of COPD • Garcia-Pachon, Prim Care Respir J 2004 • Early identification of COPD: Although SaO2 levels correlated with FEV1 pulse oximetry is not a useful test for the selection of patients for screening spirometry • With a cut-off value (SaO2<98%) they could detect 79% of COPD patients, with a specificity of 37% • 23% with significant COPD (FEV1<50%) had normal SaO2 (SaO2>95%)
Screening patients with COPD for LTOT using pulse oximetry • LTOT for > 15 hours a day increase life expectancy and quality of life in COPD patients with servere hypoxia • Over a 12-month period 114 patients with COPD were screened with pulse oximetry in two practices with a combined list size of 15742 • 13 had SaO2<92% and went to hospital for arterial blood gas analysis • 3 had PaO2<7,3 kPa and received LTOT • SaO2<92% is the cutt off point for selecting patients who require arterial blood gas analysis. Sensitivity 100% an specificity 69% in detection of PaO2<7,3 kPa. Oximetry has a valuable role in the selection of patients who need definitive arterial blood gas analysis
Acute exacerbations of COPD • Oxygen saturation measured by pulse oximetry can not replace analysis of an arterial blood gas sample • But pulse oximetry can be an effective screening test for systemic hypoxia (PaO2<8 kPa) • Patients with SaO2<92% should have arterial blood gases preformed • DSAM clinical recommendation on COPD SaO2 <90% => consider hospitalizing
Patients with acute respiratory problems or dyspnoea of unknown cause • A supporting tool alongside history and examination when managing patients with acute dyspnoea or dyspnoea of unknown cause in general practice – can be used as a red flag • Routine use of pulse oximetry in patients suspected for pneumonia can detect clinically unrecognized hypoxaemia • A study found that 10% of the patients with a pneumonia where hypoxic • A study concluded that pulse oximetry was not a useful method of excluding pneumonia in infants and should not influence the decision to obtain a CXR
Case 3 • 60 year-old woman, history of astma, visit her GP • 2 days with coughing, dyspnoea, pain in the left side of the thorax when coughing • Afebril, normal skin colour, normal heart & lung stethoscopy, puls 76, CRP<10, normal EKG • Diagnose?
Future uses of pulse oximetry in primary care • In patients with DM lower-extremity arterial disease is common and under diagnosed • Pulse oximetry of the toes was found to be as accurate as the ankel-brachial index to screen for LEAD in pt.’s with DM • Pulse oximetry of the toes was considered abnormal if the SaO2 was more than 2% lower from the finger • A combination of the two test was found to increase sensitivity from PO 77% (ABI 63%) to 86%
Conclusion • Non-invasive, simple, valide, low-costed method of monitoring SaO2 • Oxymetry in primary care help in the assessment of hypoxia and in identifying unsuspected hypoxia • It does have numerous indications • Assessment for LTOT in patients with COPD (SaO2<92%) • Exacerbations of COPD (obs SaO2<92%) • Acute severe asthma in children and adults • Other acute respiratory problems e.g. pneumonia • Dyspnoea of unknown cause • Pulse oximetry has some limits • Cannot distinguish between different forms of haemoglobins e.g. carboxyhaemoglobin • Reduced perfusion e.g. cold, cardiac failure • Nail vanish and paint