Download
1 / 100
1.03k likes | 1.26k Views
Musculoskeletal and Nervous System Review. Felix Hernandez, M.D. Muscle Tissue. Skeletal Muscle Cardiac Muscle Smooth Muscle. Skeletal Muscle. Long cylindrical cells Many nuclei per cell Striated Voluntary Rapid contractions. Cardiac Muscle. Branching cells

E N D
Musculoskeletal and Nervous System Review • Felix Hernandez, M.D.
Muscle Tissue • Skeletal Muscle • Cardiac Muscle • Smooth Muscle
Skeletal Muscle • Long cylindrical cells • Many nuclei per cell • Striated • Voluntary • Rapid contractions
Cardiac Muscle • Branching cells • One or two nuclei per cell • Striated • Involuntary • Medium speed contractions
Smooth Muscle • Fusiform cells • One nucleus per cell • Nonstriated • Involuntary • Slow, wave-like contractions
Muscle Contraction Summary • Nerve impulse reaches myoneural junction • Acetylcholine is released from motor neuron • Ach binds with receptors in the muscle membrane to allow sodium to enter • Sodium influx will generate an action potential in the sarcolemma
Muscle Contraction Continued • Action potential travels down T tubule • Sarcoplasmic reticulum releases calcium • Calcium binds with troponin to move the troponin, tropomyosin complex • Binding sites in the actin filament are exposed
Muscle Contraction Continued • Myosin head attach to binding sites and create a power stroke • ATP detaches myosin heads and energizes them for another contraction • When action potentials cease the muscle stop contracting
Isometric Contraction • Produces no movement • Used in • Standing • Sitting • Posture
Isotonic Contraction • Produces movement • Used in • Walking • Moving any part of the body
Neurogenic Atrophy • Transection of the larger nerves can be repaired if the proximal part of the axon is preserved. • The nerve distal to the transection injury degenerates (wallerian degeneration). • Fiber type grouping is seen. Figure 20-06
Myasthenia Gravis • Autoimmune disease involving the neuromuscular junction (NMJ) • More common in women than in men • Cause unknown • In the younger age group, associated with enlargement of the thymus • Hyperplasia or neoplasia (thymoma) • Striated muscles histologically normal
Myasthenia Gravis Figure 20-07
Myasthenia Gravis • Reduced number of surface receptor sites for acetylcholine at the motor neural plate • Easy fatigability and muscular weakness • Small extraoccular muscles and facial muscles most often involved • Ptosis, diplopia, easy fatigability on reading, facial muscle weakness, inability to chew; all muscles may become affected
Muscular Dystrophies • Genetic defects inherited as mendelian traits • Primary muscle cell pathology • A progressive course and symptoms related to muscle wasting
Duchenne-type Muscular Dystrophy • Most common muscular dystrophy • Caused by deficiency of dystrophin • Dystrophin holds together other structural proteins, linking them to the cell membrane Figure 20-08
Duchenne-type Muscular Dystrophy • Degeneration of skeletal muscle cells with ensuing muscle weakness • Sex-linked recessive disease • Occurs only in boys • Mothers asymptomatic • Milder form—Becker’s dystrophy
Duchenne-type Muscular Dystrophy • In the early stages, individual muscle cell degeneration and loss occur. • The abnormal muscle cells have an irregular shape, granularity of cytoplasm, and centrally located nuclei. • Muscle cell loss is progressive. • Compensatory hypertrophy of viable fibers occurs. • There is ingrowth of fibrous tissue and fat cells.
Duchenne-type Muscular Dystrophy • Appearance of symptoms in preschool children • Weakness of the weight-carrying muscles of the pelvic girdle and lower extremities • Difficulty getting up from a squatting position • Deformed legs, inability to keep legs straight, contractures and deformities of the extremities • Pulmonary infections, heart failure, anemia, reduced intelligence • Early death—usually in late teens or early 20s
Tumors of Muscles and Soft Tissues • Rhabdomyosarcoma • Synovial sarcoma • Liposarcoma • Leiomyosarcoma • Angiosarcoma
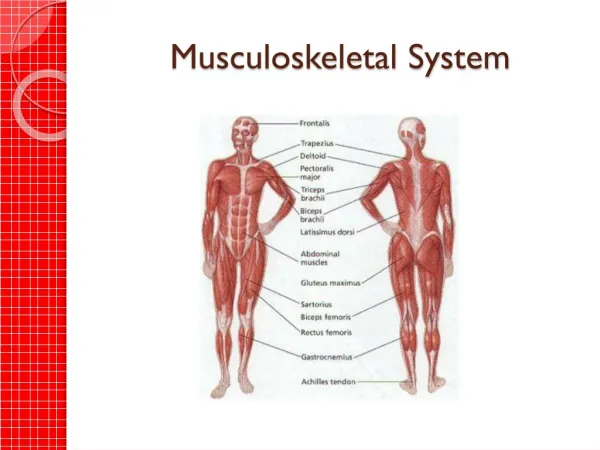
Functions of Skeletal System • SUPPORT: Hard framework that supports and anchors the soft organs of the body. • PROTECTION: Surrounds organs such as the brain and spinal cord. • MOVEMENT: Allows for muscle attachment therefore the bones are used as levers. • STORAGE: Minerals and lipids are stored within bone material. • BLOOD CELL FORMATION: The bone marrow is responsible for blood cell production.
Features of a Long Bone: Epiphysis: Ends of the bone. Diaphysis: The shaft of the bone which surrounds the medullary cavity. Articular Cartilage: Cushions the ends of the bones and allows for smooth movement. Epiphyseal Plate: Areas made of cartilage allowing for the growth of the bone.
Bone Structure • Periosteum – hard outer covering • Cells for growth and repair • Compact bone – hard strong layer • Bone cells, blood vessels, protein with Ca and P • Spongy bone – at ends of long bones • Has small open spaces to lighten weight • Marrow cavity – hollow in middle of long bones
Bone Marrow • Red marrow – produces blood cells and clotting factors • Found in humerus, femur, sternum, ribs, vertebrae, pelvis • Produces RBC 2 million per second • Yellow marrow – stores fat • Found in many bones
Haversian System • Structure of compact bone • Rings of bone tissue with blood vessels and nerves in the center
Bone Development • Initial skeleton of cartilage in infants • Replaced with bone by osteoblasts • More than 300 bones at birth – fuse to 206 • Always growing and breaking down • Osteoblasts – form new bone cells • Osteoclasts – break bone cells down • Osteocytes – mature bone cells
Osteoporosis • Multifactorial disease characterized by absolute reduction of the total bone mass • Age related—in those older than 85 years, one third have osteoporosis • Women > men, especially after menopause • Etiologically subdivided into two groups: • Primary osteoporosis—cause unknown • Secondary—related to another disease
Pathogenesis of Primary Osteoporosis • Etiology unknown, but certain factors are known to predispose to osteoporosis • Low initial bone mass (“small frame”) • Bad dietary habits, smoking • Hormones (e.g., early menopause) • Age-related changes in the metabolism
Causes of Secondary Osteoporosis • Hormonal disturbances—excess of cortisol, deficiency of sex hormones • Dietary disorders—vitamin C or calcium deficiency, malabsorption of food • Immobilization • Drugs—anticonvulsants, anticoagulants (e.g., heparin) • Tumors—breast cancer
Osteomalacia • Softening of bones as a result of inadequate mineralization of the organic matrix (osteoid) • Caused by deficiency of vitamin D, inadequate metabolic processing and activation of vitamin D, or disturbances of phosphate metabolism
Etiology of Vitamin D Deficiency • Inadequate intake—malnourished children in Africa, food faddists in United States • Inadequate exposure to sunlight—people living above the Arctic Circle • Abnormal intestinal absorption
Pathology of Osteomalacia • Excess nonmineralized osteoid • Bone deformities and fractures • Rickets = osteomalacia in children • Bowlegs • Widened costochondral junction (“rachitic rosary”) • Craniotabes • Delayed dentition
Paget’s Disease • Common chronic disease of unknown etiology characterized by irregular restructuring of bone and subsequent thickening and deformities of bones • Diagnosis made radiologically • Three phases • Destructive phase • Mixed phase • Osteosclerotic phase
Paget’s Disease • (1) In the first stage, there is irregular osteoclastic resorption of bone; • (2) In the second stage, osteoblasts react by actively laying down new bone, which balances the osteolysis and maintains the total bone volume. The disease can be recognized at this stage by the irregular manner in which osteoblasts lay down trabeculae. The new bone is highly vascular; • (3) Finally, there is a sclerotic phase in which osteoblastic activity is greatly in excess of osteoclastic resorption, leading to marked thickening of bony trabeculae and cortex
Paget’s Disease Figure 19-07A
Fractures Figure 19-08
Bone Tumor • Malignant tumors • Osteosarcoma • Chondrosarcoma • Ewing’s sarcoma • Benign tumors • Osteoma • Chondroma • Fibroma • Giant cell tumor (benign in most cases but may recur)
Osteoarthritis—Degenerative Joint Disease (DJD) • Most common joint disease • Disease of old age • Affects weight-bearing big joints but also small joints of hands and feet • Classified as: • Primary—cause unknown or multifactorial • Secondary—related to another disease
Osteoarthritis Figure 19-14
Osteoarthritis • Crepitus is a characteristic feature—a grating sound produced by friction between adjacent areas of exposed subchondral bone. • Osteophytes may be visible clinically—as bony masses such as those that occur over affected distal interphalangeal joints (Heberden's nodes)
Rheumatoid Arthritis • Chronic systemic disease of unknown etiology characterized by the following: • Chronic, symmetric inflammation of joints • proximal interphalangeal joints • Involved joints are swollen, painful, and stiff. Stiffness is maximal in the morning after the joint has been inactive during the night • Significant, but not diagnostic, laboratory findings indicative of immune disorder • Variable extra-articular findings
Rheumatoid Arthritis Figure 19-15
Rheumatoid Arthritis—Clinical Features Figure 19-16