Download
1 / 32
570 likes | 1.36k Views
Cerebrospinal fluid . Introduction. Cerebrospinal fluid (CSF) is a clear, colorless liquid that fills the ventricles (cavities) of the brain and the spinal cord. CSF replaces lymph in the CNS. The total quantity of CSF is about 150 mL, approx. 30 ml in the spinal cord.

E N D
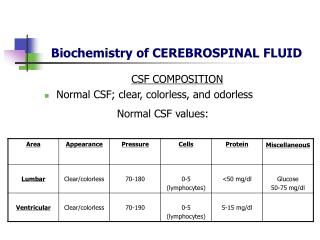
Introduction • Cerebrospinal fluid (CSF) is a clear, colorless liquid that fills the ventricles (cavities) of the brain and the spinal cord. • CSF replaces lymph in the CNS. • The total quantity of CSF is about 150 mL, approx. 30 ml in the spinal cord. • It is formed at the rate of about 0.35 ml per min OR 500 ml per day
Functions of the CSF • The CSF is believed to be nutritive for both neurons and glial cells. • The CSF provides a medium for removing waste products of cellular metabolism form the nervous system. • The presence of a number of biologically active principles (releasing factors, hormones, neurotransmitters, metabolites) within the CSF suggests that it may function as a transport system
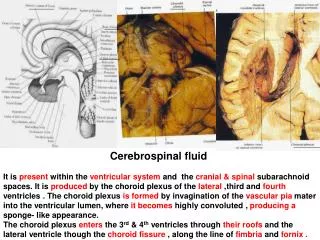
CSF Formation • The bulk of CSF is formed by the Choroid plexuses of lateral ventricles and lesser amount by the Choroid plexuses of third and fourth ventricles. • Possibly, it is also formed by Ependymal lining of ventricular system and the capillaries on the surface of brain and spinal cord
CSF Absorption • Through the Arachnoid villi, a protrusion of arachnoid membrane into the central venous sinus and other sinuses • A valve opens when CSF pressure exceeds venous pressure • Absorption by veins and capillaries of CNS
Purpose of CSF Analysis • The purpose of a CSF analysis is to diagnose medical disorders that affect the central nervous system. • Diagnostic • Viral and bacterial infections, such as meningitis and encephalitis . • Tumors or cancers of the nervous system. • Bleeding (hemorrhage) around the brain and spinal cord. • Multiple sclerosis: a disease that affects the myelin coating of the nerve fibers of the brain and spinal cord. • Syphilis, a sexually transmitted disease .
Therapeutics • Treatment • Obstructive hydrocephalus • Drug administration • Anesthesia • Antibiotic • Chemotherapy
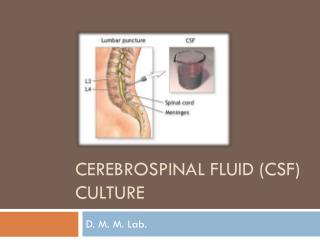
Lumbar Puncture • Lumbar puncture is used to obtain a sample of cerebrospinal fluid (CSF) to aid in the diagnosis or the therapeutic of various conditions.
LP in adults and in older children may be performed from L2 to L3 interspace to the L5 to S1 interspace. • At birth, the cord ends at the level of L3. • LP in infant may be performed at the L4 to L5 or L5 to S1 interspace. • Sterile gloves MUST be used. • Wash back with antiseptic solution. • The skin and deeper subcutaneous tissue are infiltrated with local anesthetic.
Tube 1 is used for determining protein and glucose • Tube 2 is used for microbiologic and cytological studies • Tube 3 is for cell counts and differential • Tube 4 reserve tube for any special tests
Complications • Headache • Headache After Lumbar Puncture • Most common complication, occurs 5-30% of all spinal taps, usually starts up to 48 hours after to procedure. • Usually lasts 1-2 days. • Caused by leaking of fluid through dural puncture site. • Treatment: fluids, caffeine. • Other complications • Cardio-respiratory compromise • local or referred pain • bleeding, infection • subarachnoid epidermal cyst
Opening Pressure • Normal opening pressure is • 90~180mmH2O in adults • 10~100mmH2O in children. • In Obese pts: up to 250mmH2O can be normal. • Elevated pressure • Congestive heart failure • Meningitis • Superior vena cava syndrome • Cerebral edema • Mass lesion Decreased pressure • Spinal-subarachnoid block • Dehydration • Circulatory collapse • CSF leakage
Macroscopic examination • Appearance • Normal CSF is crystal clear and the consistency of water. • The major terminology used to describe CSF appearance includes crystal clear, cloudy or turbid, milky, xanthochromic, and bloody.
Cloudy, turbid or milky • May be caused by WBCs (over 200 cells/µl). • RBCs (over 400 cells/µl) • Microorganisms (bacteria, fungi, amebas) • Specific gravity: 1.006 – 1.008 • pH: Alkaline • Spontaneous clotting • Clotting occurs when there is an excess of fibrinogen in the specimen, usually associated with a very high protein concentration. • This finding occurs classically in association with tuberculous meningitis or with tumors in CNS.
Microscopic examination • CSF cell count • Normal CSF RBCs are less than 5/mm3. • Counts that are otherwise unexplained may be due to a traumatic tap. • The cell count that is routinely performed on CSF specimen is the WBC's count. • NOTE: Cell counts should be done within 30 minutes after withdrawal of the specimen to avoid cell disintegration. • Specimen that can't be analyzed immediately should be refrigerated. • Normal adult CSF contains 0 to 5 WBC's /µl. • The number is higher in children and as many as 30 WBC's /µl can be consider normal in newborns.
Causes for increased Neutrophils • Meningitis (Bacterial meningitis, Early viral meningoencephalitis). • Reaction to repeated lumber puncture. • Injection of foreign materials in subarachnoid space. • Causes for increased Eosinophil • Parasitic infestations. • Fungal infection. • Rickettsial.
Xanthochromic • Xanthochromia is a term used to describe CSF supernatant that is pink, orange or yellow. • Pink: very slight amount of oxyhemoglobin • Orange: heavy hemolysis • Yellow: conversion of oxyhemoglobin to unconjugated bilirubin • It may be caused by the following: • Oxyhemoglobin: from lysed RBCs present in CSF before lumber puncture, or traumatic tap with lysis of RBCs after lumber puncture. • Bilirubin from lysed RBCs in CSF, or increased direct bilirubin with normal blood-brain barrier, or in premature infants an immature blood-CSF barrier plus elevated total bilirubin.
CSF protein levels over 150 mg/dl or traumatic tap with sufficient plasma concentration to produce protein concentration over 150 mg/dl. • Carotenoids in CSF due to systemic hypercharotenemia. • Bloody: grossly bloody CSF can be an indication of subarachnoid hemorrhage, but it also may be due to the puncture of a blood vessel during the spinal tap procedure.
We can differentiate between both by: • Uneven distribution of blood: Traumatic tap often shows significant clearing of blood between the first and third tubes. • Centrifugation: Traumatic tap often shows significant clear supernatant after centrifugation. • Clot formation: Fluid collected from traumatic tap may form clots due to the introduction of plasma fibrinogen into the specimen.
Glucose • Glucose enters the CSF by active transport across the blood-brain barrier. • The CSF glucose concentration is slightly lower than that plasma and usually between 60 – 70 % of plasma glucose concentration. • The normal range of CSF glucose is between 50 and 80 mg/dl • The blood glucose sample is needed for comparison. • Ideally the blood glucose sample should be drowning at least 30 min. before the lumber puncture to allow time for equilibrium between the blood and the fluid.
Clinical significance: • Low CSF glucose values can be of considerable diagnostic value in determining the causative agents in meningitis. • The finding of markedly decreased CSF glucose accompanied by: • An increased WBC's count and a large percentage of Neutrophil is most indicative of bacterial meningitis. • WBC's count and a large percentage of lymphocytes is most indicative of tubercular meningitis.
Proteins • The most frequently performed chemical test on CSF is the protein determination. Normal CSF contains a very small amount of protein. • Normal CSF protein concentration (mg/dl) is less than 1% of serum protein concentration (g/dl) and usually listed as 15 to 45 mg/dl with slightly higher values found in infants and elderly people. • A rise in CSF protein is seen in various diseases as a result of three primary mechanisms: • Decreased clearance of normal protein from the fluid and degeneration of neural tissue. • Increased local synthesis of immunoglobulin. • Increased capillary permeability due to the blood-brain barrier damage.
CSF Lactate • Measurement of lactate concentrations in cerebrospinal fluid (CSF) may be useful as part of the investigation of inborn errors of metabolism in which lactic acidosis occurs. • This includes disorders of gluconeogenesis, pyruvate dehydrogenase complex, the Krebs cycle and the mitochondrial electron transport chain. • Normal rang: 1.1-2.4 mmol\L • In bacterial, tubercular and fungal meningitis elevations of CSF lactate greater than 25mg/dl. • Destruction of tissue within the CNS owing to oxygen deprivation (hypoxia) causes the production of increased CSF lactic acid levels.
Microbiology test • Bacterial Infections • The Gram stain is of great importance, because this often dictates the initial choice of antibiotic. • Gram-negative diplococci intracellular or extracellular are indicative of Neisseria meningitidis • Small Gram-negative bacilli may include Haemophilus influenza, especially in children. • Gram-positive cocci indicates Streptococcus pneumoniae, other Streptococcus species, or Staphylococcus.
Serologic testing • Serologic testing of the CSF is performed to detect the presence of neurosyphilis. However, detection of the antibodies associated with syphilis in the CSF still remains a necessary diagnostic procedure. • Serologic tests: • VDRL (Venereal Disease Research Laboratory ) • FTA –ABS (Confirmatory test )


![CEREBRAL CIRCULATION AND CEREBROSPINAL FLUID [CSF]](https://cdn2.slideserve.com/4005143/slide1-dt.jpg)