Download
1 / 22

E N D
Beta-blockers in COPD: A systematic review based on recent research Xiao-Fang Li, Yi-Min Mao⁎Department of Respiratory Medicine, The First Affiliated Hospital/College of Clinical Medicine of Henan University of Science and Technology, Luoyang, Henan Province,China Dibacakan : dr. Chandra Kurniawan Pembimbing : dr. J.C. Matheos, Sp.P (K)
Introduction • Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease characterized by restricted airflow. • COPD is a common and frequently-occuring disease in respiratory diseases, with high morbidity and mortality. In 2015, approximately 15.5 million adults in the U.S. are diagnosed with COPD, and three million people worldwide die of COPD, an increase of 11.6% compared to 1990, and the prevalence of COPD has also increased by 44.2%. • Due to the progressive decline of pulmonary function, it seriously affects patients’ labor and quality of life, causing a huge economic burden to the world, accounted for 2.6% of the global burden of disease in 2015. COPD is expected to be the third leading cause of death in 2020.
Introduction Common clinical complications of COPD include : metabolic syndrome,sleep apnea, heart failure (HF), ischemic heart disease, pulmonary hypertension, etc. Compared to patients without HF, • COPD with HF have an estimated mortality hazard ratio (HR) of 1.3 – 1.9, • the HR of concurrent ischemic heart disease (IHD) is 1.27 – 1.5, • the HR of concurrent AF/flutter was 1.56 Because COPD and CHF overlap in symptoms and signs, as a result, patients who have a combination of the two are not fully recognized in the clinic, and missed diagnosis may occur. Most patients with CHF and COPD are not diagnosed, and vice versa.
Introduction • During the pathophysiology of CHF, the sympathetic nerve activity is compensated, and the levels of catecholamines in the blood continue to increase, causing damage to the cardiovascular system of the body. • Beta-blockers can antagonize excessive sympathetic nerve activity and affect multiple aspects of the pathophysiology of CHF to exert therapeutic effects, in accordance with the fact that β-blockers have become the main drugs in the treatment of CHF (and are strongly recommended by the North American and European heart failure treatment guidelines). • However, the treatment of COPD relies on beta-adrenergic receptor agonists, as opposed to the treatment of CHF. Previous research conclusions about the application of β-blockers in patients with COPD have been contradictory. Therefore, this article reviews the application of β-blockers in COPD based on the latest randomized controlled studies.
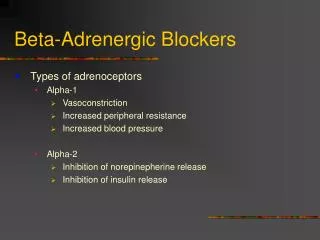
Beta-adrenergic Receptors & Beta-adrenergic Blockers Beta-adrenergic receptors are G protein-coupled receptors, which are divided into three subtypes: β1, β2, and β3 are mainly distributed on myocardial cells. • β1 receptor activation can have a positive effect on the myocardium, leading to a series of responses to myocardial excitation, such as: increased contraction, faster ejection of the heart, increased heart rate, etc. • β3 receptor activation can produce negative inotropic effects, which may be involved in the pathophysiology of HF, through inhibitory G proteins, and may also be mediated through nitric oxide pathway. • Β2 receptors are mainly distributed on smooth muscles, such as vascular muscles, digestive tract smooth muscles, bronchial smooth muscles, etc., and this receptor can cause smooth muscle relaxation after activation. The density of β receptors in the trachea, bronchi, and lung tissue is uneven. In the subsegmental bronchus and lung parenchyma, the total density of β2-adrenergic receptors is 2 and 4 times the density of cholinergic receptors in the same region, respectively. Β1-adrenoreceptor can also be detected in the lung parenchyma, but non in the bronchi. Therefore, different types of β-blockers have different roles in the broncho-lung tissue and produce different clinical manifestations.
Beta-receptor blockers can selectively bind to beta receptors and competitively block the binding of beta receptor agonists to beta receptors, antagonizing effects produced by beta receptor activation. According to different receptor subtypes, β-blockers can be divided into : • Non-selective β-blockers : block β1 and β2 receptors (propranolol, carvedilol) • Cardiac selective β-blockers : more selective for cardiac β1 receptors, weaker blocking effects on β2 receptors at therapeutic doses, minor adverse reactions such as bronchospasm. These drugs can be divided into β1 receptor blockers without intrinsic sympathomimetic activity (metoprolol and atenolol) and β1 receptor blockers with intrinsic sympathomimetic activity (acebutolol, cerilol) Blockade of cardiac β1 receptors by cardiac selective beta blockers is relative. For example, the ratio of β1/ β2 blocking by metoprolol is 2:1, and bisoprolol and nebivolol is about 14:1 and 45:1 respectively. Beta-receptor blockers inhibit the excitatory effect of catecholamines on the cardiac β1 receptor and the activation of the RAAS, play its role in lowering blood pressure, reducing heart rate, inhibiting cardiac neuroendocrine activation and improving cardiac function, thereby reducing mortality and improving quality of life in patients with HF.
Efficacy, Safety, and Tolerability of β-blockers in Patients With COPD • A third of COPD deaths can be attributed to cardiovascular disease; for every 10% decrease in FEV1 the risk of cardiovascular death increases by 28%. • Despite increasing evidence that beta-blockers are safe, and may be beneficial for patients with COPD, the use of beta-blockers in this population is still limited, and most large-scale clinical trials of CHF have excluded patients with COPD. This is a common phenomenon, mainly concerned that β-blockers may cause respiratory function deterioration in patients with COPD. • The American and European Cardiology Association guidelines point out that β-blockers are not prohibited in patients with COPD, and mild deterioration of clinical symptoms and pulmonary function should not be discontinued immediately, can be gradually increased from low doses.
Effect of β-blockers on Pulmonary Function • A meta-analysis of 22 RCT studies concluded that cardiac selective β-blockers have no significant adverse effects on lung function, clinical symptoms, and response to β2 receptors in patients with COPD. • 11 of the included studies were single-dose treatments. Results : compared with the placebo group, the cardiac selective β-blockers were not associated with changes in FEV1, and there were no increases in respiratory adverse reactions in the treatment group. • Another 11 studies conducted long-term comparative observations (ranging from 2 days to 16 weeks). Results : there was no significant difference in FEV1 between two groups. FEV1 in the treatment group was 1.81 + 0.72L, and FEV1 in the control group was 1.80 + 0.73L. The treatment group did not cause adverse respiratory reactions due to cardiac selective β-blockers. In addition, cardiac selective β-blockers did not affect the response of COPD patients to β2 receptor agonists. This meta-analysis has significant limitations, with some studies being single-blind and others lacking a true placebo control.
Effect of β-blockers on Pulmonary Function • Another meta-analysis in 2012 included a total of 5 randomized controlled trials, 4 of which evaluated the effects of cardiac selective and non-selective β-blockers on FEV1 in patients with COPD, and 1 evaluated only cardiac selection β-blockers. Results : non-selective β-receptor blockers reduced FEV1 by 0.14L, and selective β-receptor blockers decreased FEV1 by 0.03L. After nonselective β-blocker treatment, FEV1’s response to β-receptor agonists was reduced by 13.42%, there was no significant change in the response of FEV1 to β-agonists after cardiac selective beta-blockers, subgroup analysis of patients with cardiovascular disease also reached the same conclusion. The authors believe that beta-blockers, especially cardiac selective beta-blockers, should not be banned from use in patients with COPD.
Effect of β-blockers on Pulmonary Function • Short et al. conducted a large retrospective study involving 5977 people in order to explore the role of β-blockers in the treatment of COPD. Results : no significant relationship was found between β-blocker use and FEV1 reduction during an average follow-up of 4.35 years. Compared with the control group, the use of β-blockers can reduce all-cause mortality by 22%, while reducing the use of oral glucocorticoids and the frequency of hospitalizations due to respiratory diseases. • Japanese scholars retrospectively analyzed 31 patients with COPD who took β-blockers for more than one year and 72 patients who did not take beta-blockers, and assessed the annual change between β-blockers and FEV1 relationship. Results : no significant difference in FEV1 changes between the two groups (experimental group: - 7.6 + 93.5 mL/year, control group: - 4.7 + 118.9 mL/year).
Effect of β-blockers on Pulmonary Function • Maltais et al. studied the changes in pulmonary function in 557 patients with moderate to severe COPD who received β-blockers. Results : at 24 and 52 wks of treatment, the pulmonary function of the treatment group and the control group was improved from baseline, and there was no significant difference in the change in FEV1 and FVC between the two groups. At the same time, the use of β-blockers did not significantly affect the effect of bronchodilators in patients with COPD. Baseline FEV1 of the β-blocker group is higher than control group, and the proportion of Gold II patients is also higher than that of the control group. This reflects that doctors are not willing to β-blockers are used in patients with severe COPD. • Most retrospective studies have shown that cardiac selective β-blockers are safe and may be beneficial in COPD, but it cannot be ruled out that these benefits are due to the improved cardiac function of the drug.
Effect of β-blockers on Pulmonary Function • Selective and non-selective β-blockers also have different effects on pulmonary function in patients with COPD. A randomized, open-label, triple-crossover trial was performed in 2014 to evaluate the respiratory effects of carvedilol, metoprolol succinate, and bisoprolol in patients with HF and COPD. • RESULTS : No significant difference in FEV1 was found between different cardiac selective β-blockers (Metoprolol and Bisoprolol), but after switching to carvedilol (non-selective β-blockers) resulted in a significant reduction in FEV1. • Some studies have also shown that bisoprolol is less likely to cause bronchospasm than non-selective beta-blockers, and the risk can be further reduced by gradually increasing the dose in small doses.
Effect of β-blockers on The Risk of Exacerbation of COPD • A retrospective study conducted by Puente-Maestu et al. showed that the addition of β-blockers to patients with COPD with coronary heart disease or CHF can reduce the risk of acute exacerbation of COPD. Bhatt et al. conducted a prospective cohort study on whether β-blockers can reduce the worsening of COPD, including 3464 COPD patients in GOLD stage 2-4, with an average follow-up of 2.1 years. Results : risk of acute exacerbation and severe exacerbation of COPD was significantly reduced in patients receiving β-blockers (incidence risk ratio-IRR: 0.73, 95% CI: 0.60-0.90; IRR 0.67, 95% CI: 0.48-0.93). Conclusion : that β-blockers can significantly reduce the worsening of COPD regardless of the severity of airflow obstruction, but randomized placebo-controlled trials are still needed to verify this. The study did not evaluate the safety of β-blockers in patients with COPD and cardiac disease or in patients without cardiovascular disease.
Effect of β-blockers on The Risk of Exacerbation of COPD • Neef et al. conducted a retrospective study of 36 patients with acute exacerbation of COPD, and the results showed that no patients had clinically significant decline in respiratory function after starting β-blockers, including exacerbation of clinical symptoms, oxygen, bronchodilators, or auxiliary increased demand for ventilation. After 48 h of treatment, only one case (2.8%) developed symptomatic hypotension. However, the sample size of this study is small and has certain limitations. • The Maltais et al. study also showed that the proportion of acute exacerbations of COPD in the β-blocker group and the control group was basically the same. • Compared with selective β-blockers, non-selective β-blockers have a higher risk of exacerbating COPD. Compared with bisoprolol, carvedilol may aggravate respiratory symptoms by blocking β2 receptors, but due to genetic polymorphisms, carvedilol has individual effects. A cohort study in Denmark showed that carvedilol increased the risk of hospitalization in patients with CHF and COPD compared to metoprolol, bisoprolol, and nebivolol.
Effect of β-blockers on The Prognosis of COPD • A meta-analysis of an observational cohort study confirmed that β-blocker use in COPD patients not only reduces overall mortality but also reduces the risk of COPD exacerbation (OR: 0.63, 95% CI: 0.57–0.71). A meta-analysis of another cohort study reached the same conclusion. • Rutten et al. conducted an observational cohort study of 2230 patients with COPD to evaluate the effect of β-blockers on mortality in patients with COPD. The average follow-up time was 7.2 years, and they were found to be relevant after treatment with β-blockers. The hazard ratio (HR) for mortality was significantly lower (0.68, 95% CI: 0.56 to 0.83). Subgroup analysis showed similar results in patients with COPD but no significant cardiovascular disease. • Beta-blockers can improve survival and reduce the risk of death in patients with COPD and cardiovascular complications. Quint et al. evaluated the effect of β-blockers in 1063 COPD patients who were recently diagnosed with myocardial infarction (MI) and found that β-blocker therapy has a survival benefit significant impact (full adjusted risk was 0.50, 95% CI: 0.36 to 0.69; P < 0.001; median follow-up time was 2.9 years).
Effect of β-blockers on The Prognosis of COPD • Patients who took β-blocker before myocardial infarction also had a survival advantage (0.59, 0.44–0.79; P < 0.001). It shows that β-blockers can improve the survival rate of patients with COPD and myocardial infarction. • van Gestel et al. studied the relationship between cardiac selective β-blockers and mortality in patients with COPD requiring major vascular surgery, and Significant reductions in 30-day and long-term mortality were found in patients receiving cardiac selective beta blockers (OR: 0.37, 95% CI: 0.19 to 0.72; HR: 0.73, 95% CI: 0.60 to 0.88). • A retrospective study in Taiwan compared the efficacy of different beta blockers in patients with heart failure and COPD [64], and found that only high-dose bisoprolol (≥1.25 mg/day) significantly reduced the exacerbation of CHF. Betablocker use was not associated with exacerbation of COPD. In patients with combined CHF and COPD, bisoprolol reduced mortality, worsened failure, and hospitalization needs compared to carvedilol and metoprolol.
Effect of β-blockers on The Prognosis of COPD • Selective and non-selective β-blockers also have different long-term prognosis for patients with COPD. • In a retrospective study conducted by Kubota et al., total of 132 patients with decompensated HF and COPD were divided into β-blocker and non-β-blocker groups, β-blocker group is further divided into carvedilol group and bisoprolol group [65]. The primary outcome measure was all-cause mortality between the β-blocker and non-β-blocker groups (mean follow-up time was 33.9 months). • Beta-blockers reduce all-cause mortality in univariate analysis (unadjusted hazard ratio [HR]: 0.41; 95% CI: 0.17–0.99; P = 0.047). However, in multivariate analysis, there was little correlation between beta-blocker use and all-cause mortality. In addition, patients taking bisoprolol were less likely to be hospitalized again because of worsening HF and/or COPD than patients taking carvedilol.
Effect of β-blockers on The Prognosis of COPD • The authors consider the use of β-blockers to be safe in patients with COPD and HF. However, the study included a small number of people, and the retrospective study had a low degree of demonstration. Further research is needed to confirm whether there is a difference in the improvement effect of the two beta-blockers on HF and COPD patients. • Another retrospective cohort study also clearly showed that selective β1-blockers are safe during COPD exacerbation. • In contrast, an assessment of the effect of β-blockers on mortality in patients with oxygen-dependent COPD showed that β-blockers reduce patient survival. In the observation of the effects of β-blockers on elderly patients with COPD or asthma combined with acute myocardial infarction (AMI), it was found that β-blockers after AMI may be beneficial for patients with COPD or mild asthma. No survival benefit found in elderly AMI patients with severe lung disease.
Effect of β-blockers on The Prognosis of COPD A new multicenter, randomized, placebo-controlled study of β-blockers in preventing acute exacerbations of COPD. A total of 532 patients with moderate or severe COPD were randomized into a slow release metoprolol group and a placebo control group. The main observation indicators were the time of the first exacerbation of COPD during treatment, and the secondary observation indicators were the number of hospitalizations required for acute exacerbations, the frequency of adverse events and quality of life. There was no significant difference in the median time before the first episode between the two groups after the end of the treatment period. The metoprolol group was 202 days and the placebo group was 222 days (the risk ratio of metoprolol to placebo was 1.05; 95% CI, 0.84 to 1.32; P = 0.66), and there is no statistical difference in the annual acute attack rate per person between the two groups.
Pathophysiology of Beta-blockers • The pathophysiology of β-blockers is relatively complicated, and the advantages in patients with COPD are not fully reflected in the cardiovascular system. In the pathological process of CHF, due to the persistent effects of high levels of catecholamines on β receptors, the number of β receptors can be reduced, that is the β receptor downregulated. • Beta-blockers can protect β-receptors from catecholamines and help increase the number of receptors. This may be one of the benefits of β-blockers in COPD patients. • Vegh et al. used an animal model of bronchial asthma to demonstrate increased airway β2 receptor density after long-term use of β-blockers. COPD patients have an increased risk of arrhythmia. Beta-blockers block beta-receptors, which can inhibit myocardial ectopic rhythms, delay intracardiac conduction, and prevent arrhythmias. • A variety of inflammatory cells and cytokines are involved in the pathogenesis of COPD. Studies have shown that β-blockers can reduce the levels of interleukin 10 and tumor necrosis factor-α in patients with HF in dilated cardiomyopathy. This may be one of the benefit mechanisms of β-blockers in patients with COPD.
Conclusions • Beta-blockers need long-term use in the treatment of cardiovascular diseases before they can achieve therapeutic effects by changing the neuroendocrine mechanism. Adverse reactions in the respiratory system generally occur early in the medication and are positively related to the dose of the drug. • Patients with COPD can choose selective β-receptor blockers as much as possible. At the same time, they start with small doses and gradually increase to the maximum therapeutic amount according to clinical symptoms. • How to get proper treatment for patients with COPD combined with cardiovascular disease is still a continuing problem. More attention needs to be paid to cardiovascular disease specialist and respiratory department. Large-scale randomized controlled studies are still needed to verify the effectiveness and safety of β-blockers in patients with mild or severe COPD, especially patients with cardiovascular indications, as well as the optimal drug dosage and course of use, which is critical to improving patient outcomes and quality of life.