Download

1 / 30
310 likes | 672 Views
SYMPATHOLYTIC AGENTS Beta Receptor Blockers. BETA-ADRENERGIC RECEPTOR BLOCKERS. Widely used clinically for a variety of conditions ; mainly CVS Dichloro-isoproterenol (DCI) – 1 st selective -blocker Propranolol – 1 st to come in wide use – prototype agent .

E N D
SYMPATHOLYTIC AGENTS Beta Receptor Blockers
BETA-ADRENERGIC RECEPTOR BLOCKERS • Widely used clinically for a variety of conditions ; mainly CVS • Dichloro-isoproterenol (DCI) – 1st selective -blocker • Propranolol – 1st to come in wide use – prototype agent
Subsequent agents differ in terms of: • Selectivity for 1 or 2 • Intrinsic sympathomimetic activity - partial agonist activity • Membrane stabilising property - local anaesthetic property • Additional actions - on -receptors, vasodilatation, free-radicals • Lipid solubility and pharmacokinetics
GENERAL PHARMACOKINETIC PROPERTIES Mostly well absorbed orally Most agents undergo first pass effect – variable bioavailability (exceptions:betaxolol, sotalol, pindolol) Most agents rapidly distributed - with large Vd Metabolized in liver (Cy P450) Exception: Nadolol (excreted unchanged) Propranolol is highly lipophilic – readily crosses BBB T ½ between 3 to 10 hrs for most agents – Esmolol – 10 minutes – Nadolol – 24 hours
PHARMACOLOGICAL ACTIONS Can be explained on basis of knowledge of -receptor actions in tissues • EFFECTS ON CVS • Antiarrhythmic • Antianginal • Antihypertensive
CVS Effects on Heart : HR and contractility – Marginal in resting state. Exercise induced minimized Initially: CO, peripheral resistance (reflex) Continued use: symp. tone returns to normal or Prevent exercise-induced ↑ in HR and contractility Tend to limit work capacity 2 block in arteries limits in muscle bl. flow Blunt CA induced in glucose metabolism
Rhythm and Conductivity sinus rate rate of spontaneous depolarization CV in atria and AV node; ERP of AV node ( Membrane stabilizing effects may also contribute to antiarrhythmic effect of some members like propranolol) ANTIARRHYTHMIC
Effect on coronary blood flow : • myocardial oxygen demand important for anti-anginal action ( improve relationship between oxygen demand and supply) ANTI ANGINAL
Anti-hypertensive effects No marked effect in normal in hypertensives Sites/mechanisms: HR and contractility renin release from J-G cells (1 receptors promote) presynaptic 2 receptors Central actions Additional effects in some blockers ( blockade, intrinsic activity) ANTIHYPERTENSIVE
Actions on Pulmonary System Non selective blockers --- No marked effect in normal Bronchospasm in asthmatics, COPD 1-selective less likely to cause this effect but to be used with caution
EFFECTS ON EYE Several agents reduce intraocular pressure Especially in Gluacoma Mechanism : Possibly decreased aqueous formation due to decreased CyAMP in ciliary body Timolol, Betaxolol, Carteolol
Metabolic actions Carbohydrates ↓ gluconeogenesis & glycogenolysis Non-selective blockers recovery from hypoglycaemia in IDDM (1-selective agents preferable – less likely to cause this effect) Block the warning signals of hypoglycaemia Not much effect on insulin release
Metabolic actions Fat Attenuate release of FFA from adipose tissue (3) Modest in plasma triglycerides and in HDL (? Undesirable) 1 selective – lesser action on lipid metabolism Agents with intrinsic activity possibly better
Other effects Block CA induced tremor(Propranolol) Block inhibition of mast cell degranulation by CAs
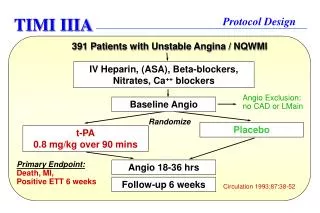
Therapeutic Uses Hypertension Ischaemic Heart Disease Angina Pectoris (not in vasospastic) Myocardial Infarction : Acute infarction: mortality (not if ↓↓ HR or BP, CHF ) Long term use: recurrence Supraventricular and Ventricular arrhythmias ↑ AV nodal refractory period Suppress ventricular ectopics
Other CVS disorders: CHF: Recent evidence: blockers may be beneficial in long term management of CHF - mortality – only metoprolol, carvedilol, bisoprolol – only in selected cases β blockers are generally contraindicated in CHF ↑ stroke volume in hypertrophic cardiomyopathy – decreased ventricular rate – decreased outflow resistance Dissecting aortic aneurysm – decreased rate of development of systolic pressure
Other uses: Hyperthyroidism – to control CVS signs Propranolol also inhibits peripheral conversion of T3 to T4 Migraine prophylaxis -- Propranolol, Timolol, Metoprolol Acute panic attacks and acute anxiety states Glaucoma - rate of aqueous secretion ( Timolol, Betaxolol) Pheochromocytoma – after blockade
ADVERSE EFFECTS Mainly attributable to -receptor blockade 1. CVS: CHF in susceptible pts. (compensated HF, post-MI, cardio-megaly) (prolonged low dose -blocker administration may be beneficial in selected cases) Bradycardia Partial or complete AV block --- serious brady-arrhythmias Abrupt discontinuation: exacerbates angina, sudden death.
ADVERSE EFFECTS….. 2. Due to vascular -receptor blockade Vasoconstriction – cold extremities; worsening of peripheral vascular insufficiency (eg. Raynauds ) 3. Bronchospasm : In susceptible, asthmatics Can occur even with β1 selective
ADVERSE EFFECTS….. 4. CNS: Fatigue, sleep disturbances (insomnia, nightmares) 5. Metabolic effects ↑ triglycerides,↓ HDL Prolong hypoglycaemia (IDDM) Overdosage: in HR, hypotension, prolonged AV conduction, widening of QRS, depression. (Glucagon may be used as antidote)
Non-selective Blockers PROPRANOLOL : 1 = 2 + membrane stabilizing action No intrinsic activity; no blocking action Pharmacokinetic properties: Completely absorbed from GIT but extensive 1st pass (upto 75%) Variable presystemic clearance and dose requirements Highly lipophilic; 90% plasma protein bound; readily enters CNS Short t ½ (4 hrs) but antihypertensive effects fairly prolonged to enable BD dosage Extensively metabolized and excreted in urine
Propranolol…. Therapeutic Uses : Hypertension, stable angina pectoris, arrhythmias, Migraine prophylaxis, Hyperthyroidism Interactions: Phenytoin, rifampin, phenobarb - conc. CCBs (verapamil and diltiazem) – additive effects on conduction Nifedipine – positive interaction
TIMOLOL : Non-selective, no intrinsic or membrane stabilizing activity Used mainly in Glaucoma by local instillation (significant absorption may occur to cause systemic effects : adverse effects in susceptible LABETALOL: Non selective + 1 blocker + partial agonist at 2 4 isomers with relatively different proportion of the above actions Complex actions Use : Pheochromocytoma; Hypertensive emergencies
NADOLOL: Long t ½ ; once daily dosage PINDOLOL: Intrinsic activity – may be preferable in Pts with diminished cardiac reserve or propensity for bradycardia SOTALOL: Antiarrhythmic activity independent of -blocking action ( K+ Channel blockade )
1 - selective blockers (Cardioselective) ATENOLOL: No intrinsic activity Limited CNS penetration Pharmacokinetics: Incomplete oral absorption Insignificant presystemic clearance Relatively little individual variation Excreted unchanged in urine (May accumulate in renal failure) Uses: Hypertension Stable angina pectoris Isolated systolic hypertension in elderly
METOPROLOL: Completely absorbed; High first pass effect; 40 % bioavailability Extensively metabolized ; 10% excreted unchanged in urine Uses: Hypertension; Stable angina IV for Ac. MI Selected cases of CHF ACEBUTALOL: 1 selective with some intrinsic activity Uses: hypertension; ventricular arrhythmias
ESMOLOL: Very short duration of action Quick onset and quick recovery from effect Administered IV in severe acute conditions where adverse effects may necessitate quick withdrawal
Newer Agents CARVEDILOL: Non-selective + 1 blocker + anti-oxidant action BETAXOLOL : 1 selective, used in glaucoma, Less chances of bronchospasm as compared to Timolol CELIPROLOL: 1 selective + mild 2 agonist + weak vasodilator
β2 selective blocker Butoxamine β2selective blockers do not have any potential use hence not pursued for development