Download
1 / 11
110 likes | 457 Views
New Concept of DSAEK Injecting System. Takeshi Ide, MD,PhD, Terrence P. O’Brien, MD, Sonia H. Yoo, MD Bascom Palmer Eye Institiute, Miami, FL, USA. Financial Disclosure Educational Research Grant was provided by KANEKA(Osaka Japan) Takeshi Ide, MD: research for KANEKA

E N D
New Concept of DSAEK Injecting System Takeshi Ide, MD,PhD, Terrence P. O’Brien, MD, Sonia H. Yoo, MD Bascom Palmer Eye Institiute, Miami, FL, USA Financial Disclosure Educational Research Grant was provided by KANEKA(Osaka Japan) Takeshi Ide, MD: research for KANEKA TerrenceO’Brien MD: consultant for AMO, Alcon, Allergan, B&L, Inspire Pharmaceuticals, Ista Pharmaceuticals Sirion Therapeutics, and Vistakon Pharmaceuticals Sonia Yoo, MD: consultant for Alcon; research for Carl Zeiss Meditec; travel expenses by IntraLase Corpation None of the authors have a propriety interest in this study.
Abstract To report the efficacy and safety of a new DSAEK tissue injecting system in an in vitro experimental model. Three human DSAEK donor tissues were prepared and loaded into our DSAEK injecting system. The tissues were subsequently injected into balanced salt solution (BSS) and stained with alizarin red S and trypan blue. Imaging software was then utilized to identify and analyze the endothelial cell damage area. This DSAEK injecting system functioned adequately for all three donor tissues. The cell damage area was 12.98±3.13%, which was comparable or less than reported damage areas by other injecting devices. This injecting system was as safe as other reported devices with regard to cell damage. This device also can maintain the anterior chamber, inject air, and release pressure. These features could significantly enhance the safety of DSAEK.
Purpose To report the efficacy and safety of a new DSAEK tissue injection system in an in vitro experimental model.
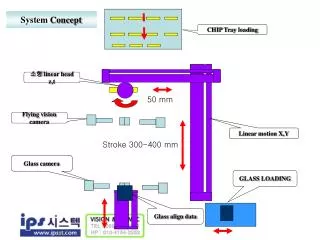
Materials New DSAEK Injection System (A) Injector Bodywith two pushers to insert donor tissues into host eyes( one pusher is for tissue injection and the other for releasing AC pressure) (B) 1ml-Syringe for injecting air into anterior chamber (AC). (C) Roller Clamp to control the flow rate of ophthalmic surgical solution (D) Balanced Salt Solution (BSS) to maintain AC. D C A B
Materials Safety mechanisms (A) Insert the nozzle part of the injector, irrigate BSS solution to maintain AC (B) Inject the tissues into the AC (C) Inject air bubble to lift up the tissues
Materials Safety mechanisms (D) Reduce IOP to avoid sudden AC collapse and the sudden ejection of the tissues from the AC as a result of the high IOP. (E) Remove the Injector, and finish tissue insertion.
Experimental Methods • Three human DSAEK donor tissues were prepared with a mechanical microkeratome • 2. The tissues were loaded onto the injector • 3. The tissues were injected into BSS • 4. The tissues were stained with alizarin red S and trypan blue. • 5. The area of cell damage was analyzed with Photoshop
A B C D E F G Methods • Injector body • (B) Hinge part • (C) Place the DSAEK tissue • (D) Cohesive ophthalmic • viscoelastic device (OVD) was • placed on the endothelial side of • the DSAEK donor tissues. Slide • the injector pusher, set the inner • cylinder over the tissue • (E) Close the hinge part • (F) Slide and tighten the hinge cover • (G) Slide the injector-pusher, • release the tissue into the BSS
Results Sample1 and three different gating conditions Sample2 and three different gating conditions Sample3 and three different gating conditions Quantitative analysis of the acute endothelial cell damage was performed by the method described by Terry et al. *18, 23
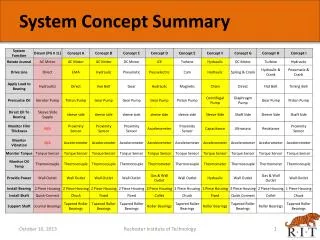
Results Table : Cell Damage Area Different Gating Conditions by 3 different corneal specialists
Conclusion • Our new DSAEK injector functioned adequately and caused a relatively small cellular damage in the in vitro model. • Our prototype has 3 safety mechanisms • A. BSS Irrigation system to keep AC • B. Air injection system to lift the tissue up • C. IOP releasing system to avoid tissue ejection • These are useful especially for surgeons who perform DSAEK occasionally, since non-volume DSAEK surgeons have difficulty in grasping and inserting the tissue using forceps on their first attempt. • 3. These features can significantly enhance the safety of DSAEK procedures, though further device modifications and ex vivo and in vivo studies are needed prior to clinical use