Download
1 / 65
710 likes | 1.07k Views
Introduction to Psoriasis. Denise Cook, M.D. Medical Officer Division of Dermatology and Dental Drug Products. Introduction to Psoriasis. Prevalence Genetics and Pathogenesis Clinical Variants of Psoriasis State of the Armamentarium. Prevalence.

E N D
Introduction to Psoriasis Denise Cook, M.D. Medical Officer Division of Dermatology and Dental Drug Products
Introduction to Psoriasis • Prevalence • Genetics and Pathogenesis • Clinical Variants of Psoriasis • State of the Armamentarium
Prevalence • Psoriasis occurs in 2% of the world’s population • Prevalence in the U.S may be as high as 4.6% • Highest in Caucasians • In Africans, African Americans and Asians between 0.4% and 0.7%
Prevalence • Equal frequency in males and females • May occur at any age from infancy to the 10th decade of life • First signs of psoriasis • Females mean age of 27 years • Males mean age of 29 years
Prevalence • Two Peaks of Occurrence • One at 20-30 years • One at 50-60 years • Psoriasis in children • Low – between 0.5 and 1.1% in children 16 years old and younger • Mean age of onset - between 8 and 12.5 years
Prevalence • Two-thirds of patients have mild disease • One-third have moderate to severe disease • Early onset (prior to age 15) • Associated with more severe disease • More likely to have a positive family history • Life-long disease • Remitting and relapsing unpredictably • Spontaneous remissions of up to 5 years have been reported in approximately 5% of patients
Genetics and Pathogenesis • Psoriasis and the Immune System • The major histocompatibility complex (MHC) • Short arm of chromosome 6 • Histocompatibility Antigens (HLA) • HLA-Cw6 • HLA-B13, -B17, -B37, -Bw16 • T-lymphocyte-mediated mechanism
Psoriasis as a Systemic Disease • Koebner Phenomenon • Elevated ESR • Increased uric acid levels → gout • Mild anemia • Elevated α2-macroglobulin • Elevated IgA levels • Increased quantities of Immune Complexes
Psoriasis as a Systemic Disease • Psoriatic arthropathy • Aggravation of psoriasis by systemic factors • Medication • Focal infections • Stress • Life-threatening forms of psoriasis
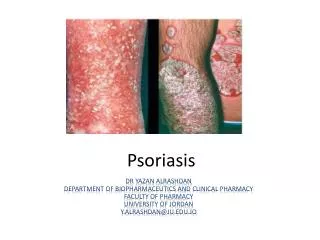
Characteristic Lesion of Psoriasis • Sharply demarcated erythematous plaque with micaceous silvery white scale • Histopathology • Thickening of the epidermis • Tortuous and dilated blood vessels • Inflammatory infiltrate primarily of lymphocytes
Severity of Disease • Three Cardinal Signs of Psoriatic Lesions • Plaque elevation • Erythema • Scale • Body Surface Area
Chronic Plaque Psoriasis • Most Common Variant • Plaques may be as large as 20 cm • Symmetrical disease • Sites of Predilection • Elbows • Knees • Presacrum • Scalp • Hands and Feet
Chronic Plaque Psoriasis • May be widespread – up to 90% BSA • Genitalia involved in up to 30% of patients • Most patients have nail changes • Nail pitting • “Oil Spots” • Involvement of the entire nail bed • Onychodystrophy • Loss of nail plate
Symptoms of Chronic Plaque Psoriasis • Pruritus • Pain • Excessive heat loss • Patient Complaints • Unsightliness of the lesions • Low self-esteem • Feelings of being socially outcast • Excessive scale
Guttate Psoriasis • Characterized by numerous 0.5 to 1.5 cm papules and plaques • Early age of onset • Most common form in children • Streptococcal throat infection often a trigger • Spontaneous remissions in children • Often chronic in adults
Life–Threatening Forms of Psoriasis • Generalized Pustular Psoriasis • Erythrodermic Psoriasis
Generalized Pustular Psoriasis • Unusual manifestation of psoriasis • Can have a gradual or an acute onset • Characterized by waves of pustules on erythematous skin often after short episodes of fever of 39˚ to 40˚C • Weight loss • Muscle Weakness • Hypocalcemia • Leukocytosis • Elevated ESR
Generalized Pustular Psoriasis • Cause is obscure • Triggering Factors • Infection • Pregnancy • Lithium • Hypocalcemia secondary to hypoalbuminemia • Irritant contact dermatitis • Withdrawal of glucocorticosteroids, primarily systemic
Erythrodermic Psoriasis • Classic lesion is lost • Entire skin surface becomes markedly erythematous with desquamative scaling. • Often only clues to underlying psoriasis are the nail changes and usually facial sparing
Erythrodermic Psoriasis • Triggering Factors • Systemic Infection • Withdrawal of high potency topical or oral steroids • Withdrawal of Methotrexate • Phototoxicity • Irritant contact dermatitis
State of the Armamentarium • Wide range of therapies for the treatment of moderate to severe psoriasis • None induce a permanent remission • All have side effects that can place limits on their use
State of the Armamentarium • Therapies • Topical Corticosteroids • Topical Vitamin D3 Analogues • Topical Retinoids • Photo(chemo)therapy • Systemic Therapies • Oral • Parenteral
Topical Corticosteroids • High potency and Super potent topical steroids • These include • Fluocinonide family (cream, ointment, gel) • Betamethasone dipropionate cream • Clobetasol propionate family (cream, ointment, gel, foam, lotion) • Diflorasone diacetate ointment • Betamethasone dipropionate ointment
Topical Corticosteroids • Side effects associated with use • Skin atrophy • Burning and stinging • Suppression of the hypothalamic-pituitary-adrenal (HPA) axis • This may occur after 2 weeks of use with certain topical corticosteroids
Topical Vitamin D3 Analogues • Prototype for this group is calcipotriene • 3 formulations – cream, ointment, and scalp solution • Former two are approved for plaque psoriasis • Latter for moderate to severe psoriasis of the scalp
Topical Vitamin D3 Analogues • Side Effects • Cutaneous • Burning • Stinging • Pruritus • Skin irritation • Tingling of the skin
Topical Retinoids • Tazarotene Gel and Cream • Available in two strengths • 0.05% and 0.1% • Side Effects • Pruritus • Burning/Stinging • Erythema • Worsening of psoriasis • Irritation • Skin pain • Hypertriglyceridemia
Topical Tazarotene • Additional Indications • 0.1% gel - approved for the treatment of facial acne vulgaris of mild to moderate severity • 0.1% cream approved as an adjunctive agent for use in the mitigation of facial fine wrinkling, facial mottled hyper- and hypopigmentation, and benign facial lentigines in patients who use comprehensive skin care and sunlight avoidance programs
Topical Tazarotene (con’t) • Both products are pregnancy category X • Are contraindicated in women who are or may become pregnant • Requirements before and during therapy • A negative pregnancy test 2 weeks prior • Therapy initiated during a normal menses • Women of childbearing potential should use adequate birth control
Photo(chemo)therapy • Two types of phototherapy • Ultraviolet B (UVB) • Ultraviolet A + psoralen (PUVA)
UVB • Two types • Broadband UVB • Narrowband UVB (311-313 nm) • Treatment is time consuming • 2-3 visits/week for several months • Side effect – possibility of experiencing an acute sunburn reaction
PUVA • Consists of ingestion of or topical treatment with a psoralen followed by UVA • Usually reserved for severe, recalcitrant, disabling psoriasis • Time consuming – 2-3 visits/wk; at least 6 weeks • Precautions • Patients must be protected from further UV light for 24 hours post treatment • With oral psoralen, wrap around UV-blocking glasses must be worn for 24 hours post treatment
PUVA • Side effects with oral psoralen • Nausea • Dizziness • Headache • Side effects with PUVA • Early • Pruritus • Late • Skin damage • Increased risk for skin cancer, particularly squamous cell (SCC) and after 200 - 250 treatments, increased risk for melanoma
Contraindications to PUVA • Patients less than 12 years of age • Patients with a history of light sensitive disease states • Patients with, or with a history of melanoma • Patients with invasive SCC • Patients with aphakia
Systemic Therapies • Oral • Methotrexate • Neoral (cyclosporine) • Soriatane (acitretin) • Parenteral • Amevive (alefacept) • Raptiva (efalizimab) • Enbrel (etanercept)
Methotrexate • Folic acid antagonist • Usually reserved for severe, recalcitrant, disabling psoriasis • Maximum improvement can be expected after 8 -12 weeks
Contraindications - Methotrexate • Nursing mothers • Patients with alcoholism • Alcoholic liver disease • Other chronic liver disease • Patients with overt or laboratory evidence of immunodeficiency syndromes • Patients who have preexisting blood dyscrasias
Methotrexate • Pregnancy Category X drug product • Contraindicated in pregnant women with psoriasis • Pregnancy must be excluded in women of childbearing potential • Pregnancy should be avoided if either partner is receiving MTX during and for a minimum of 3 months after therapy for male patients and for at least one ovulatory cycle after therapy for female patients
Methotrexate – Side Effects • Acute or chronic hepatotoxicity • Hepatic cirrhosis • Leukopenia • Thrombocytopenia • Anemia, including aplastic anemia • Rarely, interstitial pneumonitis • Stomatitis • Nausea/vomiting • Alopecia • Photosensitivity • Burning of skin lesions