Download
1 / 12
120 likes | 394 Views
“ Evaluating and Defining the Sharpness of IOLs: Microedge Structure of Commercially Available Square-Edge Hydrophobic IOLs ” Matthias Müller, PhD, 1 Liliana Werner, MD, PhD, 1,2 Manfred Tetz, MD 1 1 Berlin Eye Research Institute (BERI), Berlin, Germany

E N D
“Evaluating and Defining the Sharpness of IOLs: Microedge Structure of Commercially Available Square-Edge Hydrophobic IOLs” Matthias Müller, PhD,1 Liliana Werner, MD, PhD,1,2 Manfred Tetz, MD1 1 Berlin Eye Research Institute (BERI), Berlin, Germany 2John A. Moran Eye Center, Salt Lake City, UT, USA -The authors have no financial or proprietary interest in any product mentioned in this poster. -Supported in part by unrestricted research grants to the BERI from Alcon, AMO, Wavelight, Hoya, and Advanced Vision Science, and by a 2007 Research Grant from the ESCRS (Werner). -Some of the IOLs described here are not FDA approved.
Background • Posterior chamber intraocular lenses (IOLs) with a square posterior optic edge were found to be associated with better results in terms of posterior capsule opacification (PCO) prevention, regardless of the material used in their manufacture. This IOL design feature can be appropriately assessed in morphological studies using scanning electron microscopy (SEM). However, SEM studies of new IOLs have generally focused on the quality of their optic surface, or their optic finishing, with no specifications made on how sharp the optic edge needs to be to effectively prevent lens epithelial cells (LECs) from growing onto the posterior capsule.1 • Tetz and Wildeck performed the first attempt to evaluate and quantify the edge structure of IOLs at the microscopic level (Part 1).2 They experimentally evaluated the optimum microedge profile of an IOL to prevent LEC migration in cell culture. Experimental PMMA lenses with different edge profiles were imaged under SEM, and the area above the edge, representing the deviation from an ideal square was calculated with a digital system (EPCO).3 • The objective of this poster was to describe the findings of our current study (Part 2), for which we used an improved methodology to evaluate the optic microedge structure of currently available, hydrophobic IOLs marketed as square edge lenses. The experimental square edge PMMA lens in Part 1, with the edge design that effectively stopped LEC growth in culture was used as the reference lens against which the currently available square edge lenses were compared.4
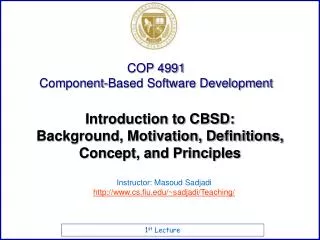
X25 X1,000 Post. surface Ant. surface (Equiconvex) In vivo LEC: 8-21 μ in diameter (larger lengths) Area = 281.4 μ2 40-μ radius Materials/Methods • IOL designs: Sixteen designs of hydrophobic acrylic or silicone IOLs. Reference square edge lens: experimental square edge PMMA lens, with an edge design that effectively stopped LEC growth in culture (Part 1). Control lenses: 2 round edge silicone lenses; • IOL powers: +20.0 D IOL and +0.0 D IOL (or the lowest available plus dioptric power); • SEM system: Hitachi S-2700 SEM (X25, X300, X1,000). Analysis from a perpendicular view of the edge; • Image analysis system: JPEG photos imported to the AutoCAD LT 2000 system (Autodesk, San Rafael, CA, USA): • Micron scale adjusted (reference bar in SEM photos); • Projection of reference circles of 40 and 60 microns of radius on the photos (the area evaluated was therefore the area of interaction of at least 1 or few LECs with the optic edge); • Area above the lateral-posterior edge (deviation from a perfect square) was measured in square microns.
Results Reference PMMA lens: 34.0 and 37.5 μ2 (40- and 60-radius circles, respectively); +20.0 D control silicone lens: 729.3 and 1,525.3 μ2; +0.0 D control silicone lens: 727.3 and 1,512.7 μ2; Acrylic IOLs: 69.5 to 338.4 μ2 (40 radius); 122.4 to 524.4 μ2 (60 radius); Silicone IOLs: 4.8 to 281.4 μ2 (40 radius); 0.2 to 520.4 μ2 (60 radius); Out of 30 lenses, 7 silicone lenses had area values smaller or in the vicinity of the corresponding values of the reference PMMA IOL (+5.0 Z9002, +20.0 L200, +20.0 SofPort AO, +0.0 and +20.0 SoFlex SE, and +12.5 and +20.0 AQ310Ai); Acrylic versus silicone lenses:P = 0.0017 for 40- and 60-radius circles (Wilcoxon Two-Sample Test); +20.0 D versus +0.0 D (or lowest available dioptric power) lenses: P = 0.4419 and P = 0.2616 (NS) for 40- and 60-radius circles.
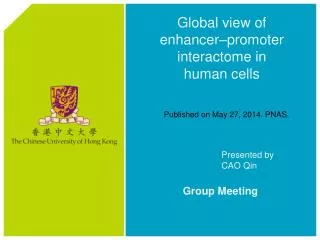
Examples of square optic edge profile and finishing of hydrophobic acrylic IOLs: Matrix Acrylic, +0.0 D SA60AT, +20.0 D Z9003, +10.0 D AR40e, +20.0 D L450, +20.0 D VA60BB, +0.0 D
IOLs with deviation areas in the vicinity to the cut off limits (or smaller) had similar values for the 40- and the 60-radius circles, while the others had a tendency to present increasing values with the larger radius, mostly as a function of the convexity of their posterior optic surface.
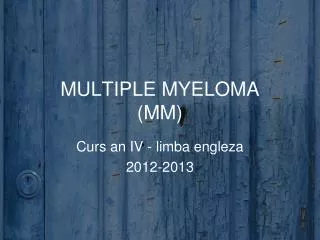
Examples of square optic edge profile and finishing of silicone IOLs: SoFlex SE, +0.0 D SofPort AO, +20.0 D Z9002, +20.0 D Z9002, +5.0 D AQ310Ai, +12.5 D Z9000, +20.0 D
Discussion / Conclusions • A square edge on the posterior optic surface was found to be the most import IOL-related factor for PCO prevention. According to different experimental studies, this may be due to the mechanical barrier effect exerted by the square edge,5 to the contact inhibition of migrating LECs at the capsular bend created by the sharp optic edge,6 to the higher pressures exerted by IOLs with a square edge optic profile on the posterior capsule,7 or perhaps to varying combinations of all of the above. • Analysis of the microstructure of the optic edge of currently available, square edge, hydrophobic IOLs revealed a large variation of the deviation area from a perfect square, as well as of the edge finishing. Both parameters varied not only among different designs, but also between different powers of the same design.
Discussion / Conclusions • If IOLs with different square microedge profiles produce similar outcomes in terms of PCO formation, one may conclude that other factors play a role in its prevention. We believe the factor that may play the most important role in even out the differences in the microedge profiles shown in our study is the shrink wrapping of the IOL by the capsular bag, enhancing the contact of the posterior IOL surface with the posterior capsule. The amount of postoperative capsular bag shrinkage has been indirectly determined in clinical studies, by the measurement of the diameter or the area of the capsulorhexis opening at different postoperative time points (13.8 to 14.8%).8-11 Central PCO = 0 Soemmering‘s ring
Discussion / Conclusions • We believe that existing and future clinical data will help us to better understand the effect of microedge structure and design on reducing PCO. At present, a cut-off value should be sought for to clinically label an IOL as square edged. This study may help on the task for better understanding differences in microedge structures. • We only focused on commercially available hydrophobic IOLs. Due to their low water content, we believe the SEM technique used did not cause any significant alteration of the IOL edge profile. Modern hydrophilic lenses, with water contents generally in the vicinity of 26% may have their microedge structure significantly modified during the vacuum required in standard SEM procedures. Therefore, we are currently evaluating the microedge structure of hydrophilic lenses by using an environmental SEM technique, which operates in low vacuum and does not require any prior coating. Results of this evaluation are the object of an upcoming report.
References • Kohnen T, Maqdowski G, Koch DD. Scanning electron microscopic analysis of foldable acrylic and hydrogel intraocular lenses.J Cataract Refract Surg 1996; 22:1342-1350. • Tetz M, Wildeck A. Evaluating and defining the sharpness of intraocular lenses: Part 1: Influence of optic design on the growth of the lens epithelial cells in vitro. J Cataract Refract Surg 2005; 31:2172-2179. • Tetz MR, Auffarth GU, Sperker M, Blum M, Volcker HE. Photographic image analysis system of posterior capsule opacification.J Cataract Refract Surg 1997; 23:1515-1520. • Werner L, Müller M, Tetz M. Evaluating and defining the sharpness of intraocular lenses: Part 2: Microedge structure of commercially available square-edged hydrophobic lenses. J Cataract Refract Surg 2008; 34:310-317. • Werner L, Mamalis N, Pandey SK, et al. Posterior capsule opacification in rabbit eyes implanted with hydrophilic acrylic intraocular lenses with enhanced square edge.J Cataract Refract Surg 2004; 30:2403-2409. • Nishi O, Nishi K. Preventing posterior capsule opacification by creating a discontinuous sharp bend in the capsule.J Cataract Refract Surg 1999; 25:521-526. • Boyce JF, Bhermi GS, Spalton DJ, El-Osta AR. Mathematic modeling of the forces between an intraocular lens and the capsule.J Cataract Refract Surg 2002; 28:1853-1859. • Gonvers M, Sickenberg M, van Melle G. Change in capsulorhexis size after implantation of three types of intraocular lenses.J Cataract Refract Surg 1997; 23:231-238. • Kimura W, Yamanishi S, Kimura T, et al. Measuring the anterior capsule opening after cataract surgery to assess capsule shrinkage.J Cataract Refract Surg 1998; 24:1235-1238. • Joo CK, Shin JA, Kim JH. Capsular opening contraction after continuous curvilinear capsulorhexis and intraocular lens implantation.J Cataract Refract Surg 1996; 22:585-590. • Hayashi K, Hayashi H. Intraocular lens factors that may affect anterior capsule contraction.Ophthalmology 2005; 112:286-292.