Download
1 / 25
250 likes | 923 Views
By: Janda Morgan April 10, 2008 Advisor: Dr Weaver Review background & statistical evidence related to childhood/adolescent obesity. Review the use of bariatric surgery in adolescents. Recommendations/conclusions regarding bariatric surgery in obese adolescents.

E N D
By: Janda Morgan April 10, 2008 Advisor: Dr Weaver
Review background & statistical evidence related to childhood/adolescent obesity. • Review the use of bariatric surgery in adolescents. • Recommendations/conclusions regarding bariatric surgery in obese adolescents.
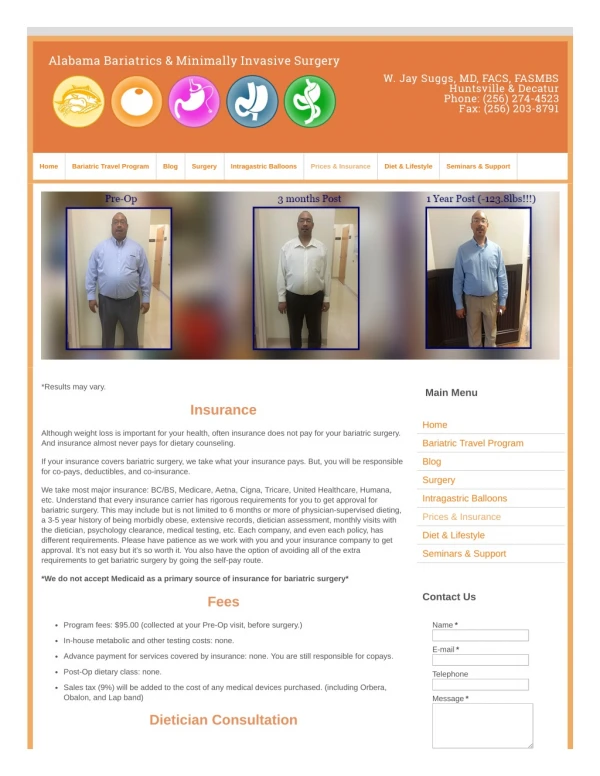
The literature varies slightly as far as the number of children/teens who are considered to be overweight/obese; however all agree that childhood obesity has dramatically increased over the past few decades. • The July 2004 journal of Pediatrics states that as many as 15-20% of adolescents are obese and 75% of those individuals will be obese adults.
Evidence indicates that the prevalence of childhood obesity is greater in the southern states. • In Kentucky, for children 5-17 years old, 43.9 percent of males and 39.3 percent of females are either at risk for being overweight or already considered to be overweight .
Childhood obesity is rarely caused by endocrine or genetic diseases. • Studies show that from 1977 to 1994, calorie consumption increased by 9 percent in adolescent boys and by 7 percent in adolescent girls. • The amount of meals eaten at restaurants or fast food stores has tripled between 1977 and 1996,and meals prepared at restaurants contain almost twice the calories as meals prepared at home.
Lack of physical activity also plays a role in childhood obesity . • Today only 6.4 percent of middle schools/junior highs and only 5.8 percent of senior highs have daily physical education programs. • Approximately 23 percent of children get no physical activity with many children spending excessive time involved in sedentary activities.
If childhood obesity trends continue the average life expectancy maybe reduced by as much as 2-5 years. • Childhood obesity is associated with the development of: Type 2 diabetes, atherosclerotic cardiovascular disease, LVH, and some forms of cancer. • An additional consequence of the increased morbidity associated with obesity is the rise in health care costs.
Roux-en-y gastric bypass • The procedure actually reduces the size of the stomach by making a small pouch that will only hold about one ounce after surgery. The pouch is created using staples and the rest of the stomach is not removed, merely separated from the pouch. • The procedure also involves making a new smaller gastric outlet, which delays the time it takes for food to leave the pouch. This new pouch will now empty into the small intestine past the duodenum. Since part of the small intestine is bypassed this causes calorie malabsorption. • The combination of a smaller stomach, decreased gastric outlet, and intestinal malabsorption allow for a much greater weight loss than seen with restrictive procedures alone.
Lap-band procedure • The procedure involves using a lap-band device that is introduced through small incisions in the abdomen and is placed around the upper part of the stomach. • This forms a small pouch without the use of stapling and results in a reduction of the functional capacity of the stomach. • There is a balloon inside the lap-band device which can be adjusted to reduce the size of the gastric outlet, which prolongs the feeling of satiety. • This procedure is restrictive only, does not have the malabsorptive component, and results in less weight loss.
Roux-en-y gastric bypass Lap-band procedure
Bariatric surgery is a major procedure that involves multiple risks and life- long post-operation implications that must be considered. • Several factors in the adolescent patient must be considered in order to decrease medical risk after surgery, maximize compliance and follow-up after surgery, and ensure adequate growth and development.
Factors for consideration in adolescent patients: • family support • the ability of the patient to make decisions • stage of linear growth reached • certain anthropometric criteria • any barriers to adherence to the post-operative regimen
The patients should have a documented attempt of at least six months of an organized weight-loss program without success. • These patients should meet the anthropometric guidelines of having a BMI of greater than 40 with the presence of a serious comorbidity (DM, HTN, sleep apnea, or hyperlipidemia). • Candidates with a BMI of at least 50 maybe considered without serious comorbidities. • These patients should have met at least 95 percent of their linear growth.
Individuals with a medically correctable cause of obesity are not candidates for surgery. • Individuals who have a history of substance abuse, psychiatric problems, or eating disorders should not have bariatric surgery. • Other exclusion criteria for the procedure include: currently pregnant, breast feeding or planning to become pregnant within one year of the surgery. • The inability or unwillingness to understand the consequences of the procedure and comply with the lifelong dietary restrictions.
Patients who undergo these procedures may suffer malnutrition and various metabolic consequences, and as a result they must comply with lifelong use of vitamin and mineral supplements. • This is of particular concern for adolescents who may not have reached their full growth potential, and research shows that adolescents have poor compliance following the post-operative dietary regimen.
Protein • Iron • Folate • Thiamine • Calcium • Vitamin D • Vitamin B12
During surgery- hemorrhage, problems with anesthesia, and bowel perforation. • Soon after surgery - pulmonary embolism, stomal stenosis, marginal ulcers, wound infections, and dehydration. • Long term complications- small bowel obstructions, cholelithiasis, or hernias.
This study showed one year post operative improvement in lab values and anthropometric data, including: BMI, TG, TC, LDL, & BG. • However 15 of the 36 patients in this study presented with complications ranging from minor complications to death. • Two of the patients began to regain weight within one year of the surgery.
This study reviewed 51 adolescents who had lap-band procedure. The results showed a mean weight loss of 42 percent of excess weight at 6 months post-op and 67 percent loss of excess weight at 18 months post-op. The study reported no mortality or other major post-op complications. The post-operative improvements include cure of diabetes or hypertension, improvement of other comorbidities, and over-all improvement of well-being. Lap banding also has the benefit of not changing the anatomy of the digestive system and the procedure is adjustable, as well as reversible if necessary. The use of laparoscopic procedures for weight loss in adolescents is promising for the future and may avoid some of the challenges associated with gastric bypass.
Address the causes of childhood obesity, including increased caloric intake and decreased physical activity. • Address the need for weight loss programs that are targeted for children & adolescents. • Practitioners need to become vigilant about assessing the weight status of their pediatric patients. • Any children who are classified as at least at risk for being overweight should have early intervention and may need referral to a dietitian.
Surgery should only be performed on individuals who meet the specific criteria outlined in this presentation. • Patients must be made aware of all of the potential risk and complications associated with this surgery. • Practitioners who are assisting adolescent patients with the decision to have bariatric surgery should make sure to research the available facilities before making referrals. Pediatric patients should only be referred to bariatric centers that have both a multi-disciplinary team and experience working with adolescent patients. • The decision to have bariatric surgery should never be taken lightly and should be made on a case-by-case basis.
Al-Qahtani AR. Laparoscopic adjustable gastric banding in adolescent: safety and efficacy. Journal of Pediatric Surgery. 2007; 42:894-897. • American Heart Association; The Robertwood Johnson Foundation. A nation at risk: obesity in the united states. • Asbs.org. [homepage on the internet]. American Society for Bariatric Surgery [updated November 23, 2005; cited October 26, 2007]. Rationale for Surgical Treatment of Morbid Obesity; [about 6 screens]. Available from: http://www.asbs.org/html/patients/rationale. • Baumer JH. Obesity and overweight: its prevention, identification, assessment, and management. Arch Dis Child Pract Ed. 2007; 92: 92-96. • Bibbins-Domingo K, Coxson P, Pletcher MJ, Lightwood J, Goldman L. Adolescent overweight and future adult coronary heart disease. The New England Journal of Medicine. 2007 Dec; 357(23): 2371-2379. • Inge T, Garcia V, Daniels S, Langford L, Kirk S, Roehrig H, et al. A multidisciplinary approach to the adolescent bariatric patient. Journal of Pediatric Surgery. 2004 Mar; 39(3): 442-447. • Inge T, Kreb N, Garcia V, Skelton J, Guice K, Strauss R, et al. Bariatric surgery for severely overweight adolescents: concerns and recommendations. Pediatrics. 2004 Jul; 114(1): 217-223. • Lawson M, Kirk S, Mitchell T, Chen M, Loux TJ, Daniels S, et al. One-year outcomes of Roux-en-Y gastric bypass for morbidly obese adolescents: a multicenter study from the pediatric bariatric study group. Journal of Pediatric Surgery. 2006 Jan; 41(1): 137-143. • Lynch R, Eisenberg D, Bell RL. Metabolic consequences of bariatric surgery. Journal of Clinical Gastroenterology. 2006 Sept; 40(8): 659-668 • Rodgers BM. Bariatric surgery for adolescents: a view from the American pediatric association. Pediatrics. 2004 Jul; 114(1): 255-256.
Singhal V, Schwenk WF, Seema K. Evaluation and management of childhood and adolescent obesity. Mayo Clin Proc. 2007; 82: 1258-1264 • Snethen JA, Broome ME, Cashin, SE. Effective weight loss for overweight children: a meta-analysis of intervention studies. Journal of Pediatric Nursing. 2006 Feb; 21(1): 45-56. • Steinbeck K. Adolescent overweight and obesity. Australia Family Physician. 2007 Aug; 36(8): 606-612. • Strauss RS, Bradley LJ, Brolin RE. Gastric bypass in adolescents with morbid obesity. Journal of Pediatrics. 2001 Apr; 138(4). Cited in mdconsult. • Stongheatlh.com. [homepage on the internet]. Bariatric Surgery Center at Highland Hospital. [Cited November 27, 2007]. Understanding bariatric surgery; [about 3 screens]. Available from: http://www.stronghealth.com/services/surgical/bariatric. • Tsai W, Inge TH, Burd RS. Bariatric surgery in adolescents. Arch Pediatr Adolesc Med. 2007 Mar; 161:217-221. • Tudor-Locke C, Kronenfield JJ, Kim SS, Benin M. A geographical comparison of prevalence of overweight school-aged children: the national survey of children’s health 2003. Pediatrics. 2007 Oct; 120(4): 1043-1050. • Xanthakos SA, Daniels SR, Inge TH. Bariatric surgery in adolescents: an update. Adolescent Medicine Clinics. 2006 Oct; 17(3). Cited in mdconsult.