Download
1 / 34
460 likes | 1.57k Views
Seborrheic Dermatitis. Rick Lin, DO MPH Texas Division KCOM Dermatology Residency Program. BACKGROUND. Seborrheic dermatitis is a papulosquamous disorder patterned on the sebum-rich areas of the scalp, face and trunk. linked to Pityrosporum ovale

E N D
Seborrheic Dermatitis Rick Lin, DO MPHTexas DivisionKCOM Dermatology Residency Program
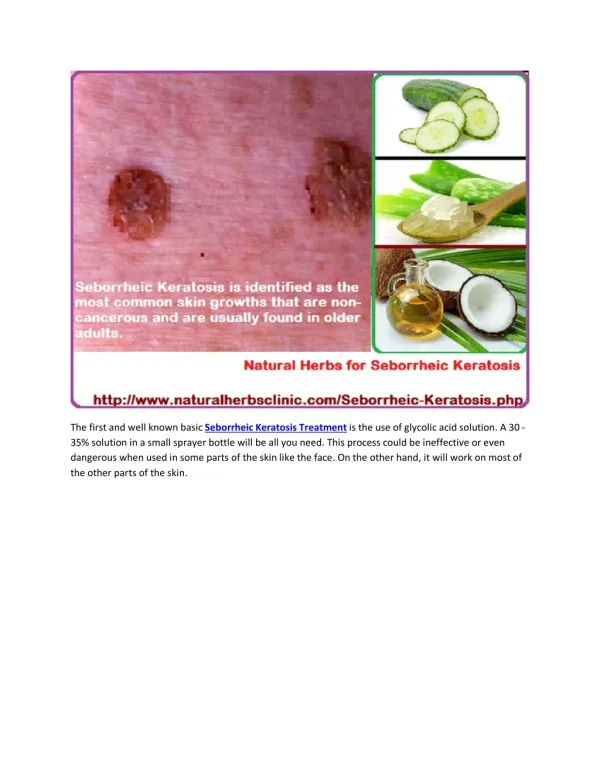
BACKGROUND • Seborrheic dermatitis is a papulosquamous disorder • patterned on the sebum-rich areas of the scalp, face and trunk. • linked to Pityrosporum ovale • immunologic abnormalities and activation of complement. • aggravated by changes in humidity, by trauma (scratching), seasonal change and by emotional stress.
BACKGROUND • Severity varies from mild dandruff to exfoliative erythroderma. • Seborrheic dermatitis may worsen in Parkinson disease and in AIDS.
BACKGROUND • Seborrheic dermatitis is associated with normal levels of Pityrosporum ovale, but an abnormal immune response. • The contribution of P. ovale may come from its lipase activity—releasing inflammatory free fatty acids (FFA)—and from its ability to activate the alternative complement pathway.
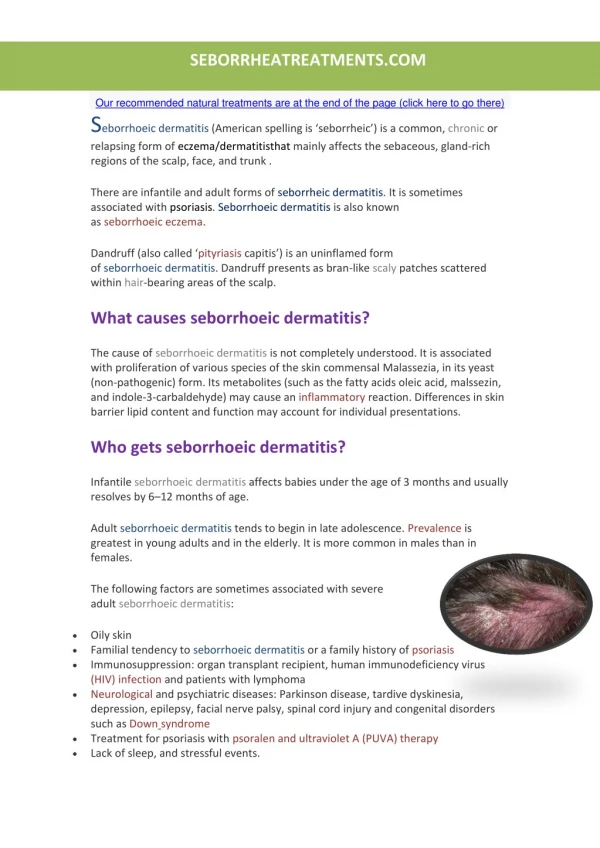
BACKGROUND • Frequency: Incidence is 3-5% with a worldwide distribution. • Race: Seborrheic dermatitis occurs in all races. • Sex: The condition is slightly worse in males. • Age: The usual onset occurs with puberty. It peaks at age 40 years and is less severe, but present, among older people. In the infant it is seen as cradle cap or uncommonly as a flexural eruption or erythroderma.
History • Intermittent active phases present with burning, scaling and itching, alternating with inactive periods. • Increased activity is seen in winter and early spring, with summer remissions common. • Active phases may be complicated by secondary infection in the intertriginous areas and on the eyelids.
History • Generalized seborrheic erythroderma is rare. It is more often seen in AIDS, CHF, Parkinson disease, and in immunocompromised premature infants.
Physical Exam • Scalp appearance varies from mild, patchy scaling to widespread thick adherent crusts. Plaques are rare. • From the scalp, seborrheic dermatitis can spread onto the forehead, posterior neck and postauricular skin, like psoriasis.
Physical Exam • Skin lesions present as branny or greasy scale over red, inflamed skin. • Hypopigmentation is seen in blacks. • Infectious eczematoid dermatitis, with its oozing and crusting, suggests secondary infection. • A seborrheic blepharitis may occur independently.
Physical Exam • Distribution follows the oily and hair-bearing areas of head and neck, such as the scalp, forehead, eyebrows, lash line, nasolabial folds, beard and postauricular skin. • Presternal or interscapular involvement is more common than the nonscaling intertrigo of the umbilicus, axillae, inframammilae inguinal fold, perineum or anogenital crease that may also be present.
Physical Exam • Two distinct truncal patterns can occasionally occur. • A rare pityriasiform variety can be seen on the trunk and neck, with peripheral scaling around ovoid patches mimicking pityriasis rosea.
Physical Exam • Pityrosporum is probably not the cause, but a cofactor, linked to a T cell depression, increased sebum and an activation of the alternative complement pathway. • As seborrheic dermatitis is uncommon in preadolescent childhood, and tinea capitis is uncommon after adolescence, dandruff in a child is more likely to represent a fungal infection. A fungal culture should be done to confirm this. (Age 6-15)
Differential Diagnosis • Asteatotic Eczema • Atopic Dermatitis • Candidiasis, Cutaneous • Contact Dermatitis, Allergic • Contact Dermatitis, Irritant • Dermatomyositis • Drug Eruptions • Drug-Induced Photosensitivity
Differential Diagnosis • Erythrasma • Extramammary Paget Disease • Impetigo • Intertrigo • Lichen Simplex Chronicus • Lupus Erythematosus, Acute • Nummular Dermatitis
Differential Diagnosis • Pemphigus Foliaceus • Perioral Dermatitis • Pityriasis Rosea • Rosacea • Tinea Capitis • Tinea Corporis • Tinea Cruris • Tinea Versicolor
Tests • A clinical diagnosis of seborrheic dermatitis is usually made by a history of waxing and waning severity and by the distribution of involvement on exam. • A skin biopsy may be needed in exfoliative erythroderma, and a fungal culture can rule out tinea capitis.
Dermatopathology • Dermatopathology of seborrheic dermatitis is nonspecific. • Hyperkeratosis, acanthosis, accentuated rete ridges, focal spongiosis, and parakeratosis are characteristic. • Psoriasis is distinguished by regular acanthosis, thinned rete ridges,parakeratosis, and an absence of spongiosis. Neutrophils may be seen in both diseases.
Medical Care • Early treatment of flares is encouraged. • 2 1/2% selenium sulfide or Nizoral (ketoconazole) shampoos may help by reducing Pityrosporum ovale scalp reservoirs. • Shampoos may be used on truncal lesions or in beards but may inflame intertriginous or facial involvement. • Neutrogena T-gel • Locoid solution.
Conclusion • Seborrheic Dermatitis mimic other papulosquamous diseases. It can look like many things • Fulminant Seborrheic Dermatitis requires additional evaluation of the immunosuppression status of the patient. • Referral to dermatologist if it just doen’t “look right”