Download
1 / 16
160 likes | 705 Views
Survey of I.V. Paracetamol use in neonates and infants under 1 year of age by UK anesthetists Elaine Wilson-Smith and Neil Morton. Pediatric Anesthesia 2009 19 : 329-337. An anecdote of error…. Busy Saturday on call, about a year ago 3.8kg 5 week old baby for pyloromyotomy

E N D
Survey of I.V. Paracetamol use in neonates and infants under 1 year of age by UK anesthetistsElaine Wilson-Smith and Neil Morton Pediatric Anesthesia 2009 19: 329-337
An anecdote of error… • Busy Saturday on call, about a year ago • 3.8kg 5 week old baby for pyloromyotomy • Doing the case solo, as the registrar had gone to help with cardiac anaesthesia temporarily • Whilst talking to surgical registrar, drew up 20mls IV paracetamol to give and starting giving slow bolus • Got to 14mls given before I realised what I was doing…..and shouldn't be! • Dose used in AH at 5/52: 15mg/kg • Dose given: 36.8mg/kg (~2.5x)
A worry? • Spoke to father, explained error and that it should have no consequence as long as no more paracetamol given until lunch time next day • Surgical registrar says "safe" to give whole day's dose in one go • We had 2 sick baby laparotomies to perform and carry straight on until 2.30 in morning • Pyloromyotomy baby is "fine" • I am not….BNFc does not reassure me (7.5mg/kg for all children under 1 year)
A worry? • I have given ~5x dose • Well known nomogram for guide to treating overdose relates to oral ingestion; IV may be worse ? • Toxbase is password protected and I can't get access • It's 3.30 in the morning, so I talk to the ICU consultant and we agree that it's best to take a blood level for the baby • Because it is now 10-11 hours post dose, we prepare to give acetylcysteine • Level comes back at 9.8mg/l – well below treatment line
Survey of i.v. paracetamol use in neonates and infants under 1 year by UK anaesthetists. Pediatric Anaesthesia 2009 • Provides some interesting data about what is known about paracetamol in this age group, which might have reassured me • UK license for IV preparation of paracetamol first included children in 2005: dose 15mg/kg TDD 60mg/kg • In June 2007, license extended to include neonates from term to up infants of 1 year or weighing 10kg, dose 7.5mg/kg TDD 30mg/kg
IV Paracetamol • Effective, well tolerated analgesic in children • 100% bioavailability, rapid peak plasma levels; peak analgesic action approx 1 hour after admin, acting centrally • Mechanisms of action reviewed by Anderson (Pediatric Anesthesia 2008 18: 915-921) • Pharmacokinetics in neonates also extensively reviewed by Anderson & Allegaert: Pediatric Anesthesia 2009 19: 289-295 • Plasma paracetamol levels 10-20mg/l are considered therapeutic
Survey of APA linkmen and members of Paediatric Pain Travelling Club Sought information regarding loading dose, maintenance dose, dosing interval Age categories<32wks, 32-36wks, 1-3 mths, 3-12 mths Factors that might prompt either stopping or tapering the use of iv paracetamol
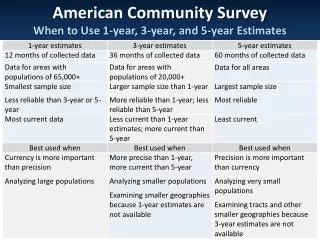
Survey results • 105 responses out of 184 individuals sent surveys • Of these 54 indicated use in children under 1 year • 45 of these gave more detailed information in younger age groups • Total daily dose of 60mg/kg is used by morethan half of respondents in 3-12mth age group • Most respondents using it in the youngest age groups used 30 mg/kg/day for babies of less than 1mth or 44wks PCA
Compliance with licensed dose • Graphs comparing doses in relation to license versus pharmacokinetic data model
Discussion • Dosing of any drug aims to deliver a therapeutic plasma or effect compartment level, whist avoiding levels that cause side effects or toxicity. • Toxicity, in the form of liver damage is a risk, but at 10x that used therapeutically* • Dosing that achieves therapeutic analgesic levels can reduce post-op opioid requirement • Lack of hepatotoxicity with regular iv paracetamol use has been demonstrated in 149 term and pre-term infants (Allegaert K et al 2008)
Paracetamol metabolism • Via glucuronidation and sulphation within the liver • In acute overdose the reactive product N-acetyl-p-benzoquinioneimine is produced • Risk factors for hepatotoxicity include: • Fasting • Vomiting • Dehydration • Systemic sepsis • Pre-existing liver disease
Paracetamol metabolism • In neonates there is a greater contribution of sulphation to metabolism, and reduced production of oxidative metabolites: this may reduce the risk of toxicity in neonates: van der Marel 2003
Important Drug Safety Information:Bristol-Myers Squibb Pharmaceuticals • May 2010 • Manufacturers of Perfalgan warn that there had been 23 worldwide cases of IV paracetamol overdose in children less than 1 year old reported • One child subsequently died • Concerns re possible confusion of prescription in mg, then administration in ml • Reiteration of licensed doses • Will departments feel that they have to change their guidelines in view of this Direct Healthcare Professional Communication?
Safer? • Errors in dosing of paracetamol (oral and IV) are common, partly because the frequency with which the drug is used • In our hospital the commonest error is of duplication (emergency department/ theatre/ward) • If the dosing error is ml for mg, this requires an education drive: each time the drug is given there is a possibility of 10x error • Errors have also occurred because of poor practice • In Sheffield, reminders posted regarding doses for different ages in syringe sizes
APA guidelines • These recommend licensed dosages. In an editorial on audits of post-op analgesia,in relation to opioid infusions and NOT referring to paracetamol dosage, Howard (Pediatric Anesthesia 2010) reminded us that protocol adherence is already used by the Patient Safety First Campaign as an outcome measure.
Paracetamol • Not licensed for oral use in children < 2/12 old • BNFc nevertheless recommends