Download

1 / 29
290 likes | 537 Views
Bio-Terrorism Overview for the Respiratory Therapist. By: UMDNJ-SHRP Respiratory Therapy Education Program Faculty. What is Bio-Terrorism?. Key Components: Advanced planning/coordination by terrorists . Strong potential for panic among lay and medical personnel

E N D
Bio-Terrorism Overview for the Respiratory Therapist By: UMDNJ-SHRP Respiratory Therapy Education Program Faculty
What is Bio-Terrorism? • Key Components: • Advanced planning/coordination by terrorists. • Strong potential for panic among lay and medical personnel • Causes a population to significantly change their routine and behavior • Potential for massive numbers of victims • Potential for mimic of endemic infectious diseases • “Medical defense against biological warfare or terrorism is an area unfamiliar to most military and civilian health care providers.” USAMRIID February 4, 2001
Historical Overview • Bio-warfare has been around since 300 B.C. via contamination of food/water and via inoculated fabrics • In 1346, Tartars catapulted bodies of plague victims over the walls of Kaffa in the Ukraine. • During the French and Indian War (1754-67), British forces gave blankets contaminated with smallpox to susceptible Indian tribes. • 1932-42: In Japan, plague infected rats were fed upon by fleas, which were released over chinese cities. • 1943: Tularemia used by Germans to disable Russians • 1982: Russians weaponize and use “Glanders” on Afghani troops • 1984:The Rajneeshee cult contaminated 10 restaurants with Salmonella in Wasco County, Oregon. • 2001: DC, NY and NJ: Anthrax attacks via mail.
High Acuity Cases Unusual “Constellation” of Symptoms Unusual or not naturally occurring disease entity Large number of cases or entities Point-source outbreak--Limited geographical areas Aerosol route Delivery High morbidity and/or mortality Low attack-rate in persons in filtered air Sentinel dead animals, esp. multiple species No natural vector Large number military and civilian casualties Indicators of Possible Bio-Attack
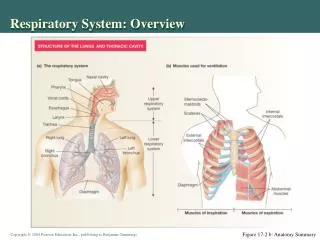
Bioterrorism: Routes of Infection • Inhalation route • Has the greatest potential for mass casualties • Aerosol dispersal most likely route • Percutaneous, e.g. anthrax as “wool sorters disease” • Oral, i.e. intake of contaminated food and water
What This Means • Respiratory Therapists will care for victims (ER, ICU) • Are Medical Personnel (RTs) Prepared?: • early recognition • innoculations: smallpox, anthrax • Isolation and barrier techniques • RTs have a responsibility to: • protect themselves & others • know how to treat these victims. • report suspicious illnesses • Prepare, Anticipate, Recognize, Act
Bioagents Most Likely to Be Used by Terrorists • Smallpox • Plague • Anthrax • Tularemia • Botulisum Toxin • Salmonella/Typhoid Fever • Q-Fever • Brucellosis • Others Agents: Staph Enterotoxin B, Ebola, Ricin (poison)
Smallpox (Variola Major) • Incubation Period: 7 - 17 days • Natural Occurrence: Last case in Somalia, 1977. • Droplet & Airborne Precautions – 17 days. Most contagious in “early rash” phase. • Presentation: Fever, backpain, vomiting, malaise, headache, rigors; papules to pustular vessicles face/ extremities. • DX: Modified silver stain, PCR and viral isolation IHC • TX: Immediate vaccination (if exposure < 5 days) and supportive care.
Pulmonic Plague (Yersinia Pestis) • Incubation Period: 1 - 6 days • Natural Occurrence: 5 - 15 cases/Yr. in US. • Droplet Precautions • Presentation: High fever, chills, hemoptysis, shock, stridor, B/S crackles, ARF. High mortality (> 75%) with late diagnoisis. • DX: Gram stain, C&S, Immunoassay for capsulated antigen • TX: Streptomycin 30 mg/kg/day IM. Oral Doxycycline or Ciprofloxin. No vaccine.
Inhaled Anthrax (Bacillus Anthraxis) • Incubation period 1-6 days up to 45 days • Natural Occurrence: Few via Inhalation. • No Known Human-to-Human Transmission • Presentation: Fever, malaise, cough, mild chest discomfort; later dyspnea, diaphoresis, stridor, cyanosis, hypotension, hemorrhagic meningitis. 50% Mortality, with treatment. • DX: Mediastinal widening w/o infiltrates on CXR, Serology, Gram stain, PCR • TX: Supportive care, Doxycycline 200 mg IV then 100 mg IV Q12 hr. Vaccine - high risk groups.
Tularemia (Francisella Tularensis) • Incubation Period: 1 - 10 days (avg. 3-5) • Natural Occurrence: 200 cases annually in US from animal sources • Human-to-Human Transmission: None known, but highly infectious via aerosol. • Presentation: fever, headache, malaise, chest discomfort, productive/non-productive cough, anorexia and conjuntival and periorbital edema. 10-20% Mortality. • DX: CXR- mediastinal lymphoadenopathy, Serology(ELISA), C&S, PCR & IHC • TX: Supportive, Streptomycin or gentamycin. No current vaccine.
Botulism (Clostridium Botulism) • Incubation Period: 1 - 5 days • Natural Occurrence: 30 cases annually • Human-to-Human Transmission: None known • Presentation: Descending paralysis, ptosis, blurred vision, diplopia, malaise, dizziness, dysarthia, and disphonia • DX: Serology, toxin assays/ anaerobic cultures of blood or stool, EMG studies • TX: Antitoxin 1 vial (10 ml) IV
Typhoid Fever (Salmonella Typhi) • Incubation Period: 2-5 Days • Occurrence: 400 cases annually in US, mostly among travelers. 21 million cases worldwide. 5% asymptomatic, but carriers (“Typhoid Mary”) • Presentation: Fever, Chills, Delerium, Malaise; Diarrhea/vomiting uncommon. • DX: Blood/stool C&S, clinical presentation, Recent history (e.g., travel). 12-30% mortality. • Tx: Antibiotics (Levaquin), supportive (Hydration), Prevention via vaccination.
Q-Fever (Coxiella Burnetii) • Incubation Period: 2-3 weeks • Natural Occurrence: Rare, but most often found in farmers; sheep/dairy workers and meat handlers. Very Resistant to Heat and environment. • Transmission: Via open wound contact with animal or dust inhalation. Very contagious via aerosol. • Presentation: 50% asymptomatic, Flu-like & GI symptoms. 1-2 week acute stage duration. Acute symptoms resolve. Chronic can develop and cause endocarditis and liver dysfunction. • Dx: Seriologic Testing for antibodies. • Tx: Antibiotics--Doxycycline & quinolones for 4 years. Vaccine in Australia, but not US.
Brucellosis (Brucella Melitenis) • Incubation Period: 5-20 Days • Natural Occurrence: 200 annually in US. • Transmission: Mainly via unpasteurized milk and contact with infected meat. Highly infectious via aerosol. • Presentation: Acute-Flu-like symptoms; Chronic- Chronic fatigue, depression • Dx: Blood C&S, Clinical presentation, Hx. • Tx: Supportive, Antimicrobials
SEB: Staphyloccocal Enterotoxin B • SEB causes symptoms when inhaled in very low doses. • Standard Precautions • Latent period: Inhalation 3-12 hrs. • Presentation: non-specific flu, non-productive cough, retrosternal pain, dyspnea. • DX: Suspicion, ELISA, PCR; no CXR abnormalities • TX: Oxygen, hydration; CMV w PEEP, vasopressors and diuretics
Ebola Hemmorrhagic Fever • Incubation Period: 2 to 21 days • Natural Occurrence: 1,000 to 3,000 cases annually, mainly in Central Africa. Isolated: 1976 • Transmission: Highly contageous via contact with blood/bodily fluids. Rarely, airborne transmission. Unknown natural reservoir! • Presentation: Early: Flu-like symptoms. Later: GI symptoms, red eyes, external/internal bleeding. • DX: Enzyme-linked Immunosorbent Assay (ELISA), Polymerase Chain Reaction (PCR). • TX: Supportive. No vaccine. 50-90% Mortality
Ricin (Poison/Toxin) • Potent poison made from waste of castor bean processing. • 500 mcg (amt. on a pinhead) is generally fatal. • Exposure is generally deliberate (G. Markov, London, 1978)…No person-to-person transmission. • Presentation: Symptoms w/I 6-8 hrs • Inhalation: Dyspnea, Cyanosis, Pul. Edema • Ingestion: GI symptoms, Seizures, Hypotension, Liver/Kidney Failure • DX: Toxicology, Recent HX, Symptoms • TX: Supportive, Discard clothes, Wash skin, No antidote!!!
Large # of people w/ similar disease/syndrome Large # of unexplained illnesses or deaths Unusual illness in population Higher morbidity / mortality Single case of uncommon agent Common denominator in all/most cases. e.g., Legionnaires Disease Epidemiologic Clues
Maintain an index of suspicion Protect thyself Assess thy patient Decontaminate PRN Establish a Diagnosis Render thy patient prompt treatment Practice good infection control Inform thy authorities Assist in Epidemiologic Investigation Maintain, Update thy proficiency & Spread the gospel. Medical Response to Bioterrorism “Ten Commandments”
What RTs Can and Should Do • Always use Protective Equipment, Especially in the ED and ICU. • Treat all critically ill medical patients as if… • Proper use of Protective Equipment: Seal mask from bridge of nose down…don’t pinch nose. • Get Educated: Understand Etiology/Pathology, Clinical Pres., Tx & Prevention of Bio-Agents • Be Aware: If It Seems Unusual, Maybe it Is!!! • Get Vaccinated!!! • Don’t Panic…Panic can be contageous too! • Don’t become another casualty!!! • Report suspicious cases per institutional protocol.
What RT Departments Can/Should Do? • Understand that another terrorist attack (Bioterrorism or otherwise) is more a question of when, not if !!! • Understand the Hospital/Organization’s Disaster Plan. • Devise an Effective Departmental Disaster Plan, consistent with that of the Organization. • Protect & Support your staff through education, as well as proper equipment and staffing. • Practice Simulated Emergency Drills.
Important Contacts: • Institutional-specific chain of command • NJ Dept. of Health & Sr. Services • 1-609-588-7500 or -3121 • 1-609-392-2020 (after hours) • NJ Poison Information and Education System • 1-800-222-1222 • NJ Office of Emergency Management • 1- 609-882-2000 • NJ Dept. of Environmental Protection • 1-877-WARNDEP (1-877-927-6337)
Take Home Messages • Educate & Prepare yourself and your staff/co-workers! • In-services, Drills, Proper Staffing & equipment • Work with your Emergency Medical and Nursing staff to develop an effective action-plan. • Conduct disaster drills on all shifts. • Be Aware and Cautious…But don’t Panic • Contact your local office of Emergency Preparedness.
Selected References • Christopher GW, Cieslak TJ, Pavlin JA, Eitzen EM. Biological Warfare, a historical prospective. JAMA. 1997; 278:412-417 • USAMRIID Medical Management of Biological Casualties Course (6H-F26) 01 February 2001 • CDC. Mandatory reporting of infectious diseases by clinicians. MMWR 1990:39(RR-9);1-11, 16-17. • National Notifiable Disease Surveillance System. Available at: http://www.cdc.gov/epo/dphsi/nndsshis. htm • National Electronic Telecommunications System for Surveillance. Available at: http://www.cdc.gov/epo/dphsi/netss.htm
Clinical Case I • You are the RT in the ER treating an dyspneic child when you overhear a mother tell the pediatrician: “I don’t understand it. My Joey had chickenpox as a preschooler and Susie had the vaccine. How could they have chickenpox? There are many really sick kids with chickenpox on their arms & legs who went to the Columbus Day parade.” The ER has had several cops with severe “chickenpox.” There was a report of an explosion at the parade. What is your suspicion? What actions would you take and recommend?
Clinical Case II • The newspaper reports that large numbers of rats are found dead. Transit workers and subway riders are in your ER complaining of dyspnea, high fevers, chills and hemoptysis. Auscultation finds bilateral crackles and stridor. • What is your suspicion? • What lab test will be helpful? • What action would you take and recommend?
Clinical Case III • A TV station reports that a terrorist group claims to have attacked Coney Island with a bioagent. Witnesses reported a cloud of white dust. As a therapist at a Brooklyn hospital you have seen numerous patients from that area with fever, headache, malaise, chest discomfort, non-productive cough and tachypnea. Exam reveals an acutely ill patient with a widened mediastinum, peripheral cyanosis and diaphoresis. • What is your suspicion? • What actions would you take and recommend? • What diagnostic test should be performed?