Download
1 / 88
950 likes | 1.52k Views
Cutaneous Manifestations of Internal Disease. Residents’ Conference Hallie McDonald, MD August 16, 2005. Diabetes Mellitus. According to Perez et al (3) ,approximately 30% of patients with DM develop skin lesions at some point

E N D
Cutaneous Manifestations of Internal Disease Residents’ Conference Hallie McDonald, MD August 16, 2005
Diabetes Mellitus • According to Perez et al (3) ,approximately 30% of patients with DM develop skin lesions at some point • Overall prevalence of cutaneous disorders does not differ between type I and type II diabetics • Type I patients get more autoimmune-type lesions • Type II patients get more cutaneous infections
Diabetes Mellitus • Cutaneous lesions usually appear after the development of DM, but may be the first presenting sign • Four major groups of skin findings • Skin diseases associated with DM (necrobiosis lipoidica and diabetic bullae) • Cutaneous infections • Cutaneous manifestions of diabetic complications (neuropathic ulcers) • Skin reactions to diabetic treatment
Necrobiosis Lipoidica (NL) • NL appears in 0.3-1.6% of diabetics (2,4) • Anywhere from 11-65% of patients with NL have DM at the time of skin dx (2,7,8) • If they do not have DM at time of dx, about 90% will develop diabetes, have abnormal glucose tolerance, or report parents with DM (2, 4) • Diabetic control has no effect on the course of NL.
Necrobiosis Lipoidica (NL) • NL is 3x more common in women. • According to Jelinek, (9) NL appears earlier (mean age 22) in Type I diabetics than Type II (mean age 49.) • Appearance • Begins as an oval, violaceous patch and expands slowly. • Advancing border is red. • Central area turns yellowish brown. • Central area atrophies and telangiectasia become evident. • 13% of cases progress to ulceration
Necrobiosis Lipoidica (NL) • Classically, NL occurs bilaterally on the pretibial or medial malleolar areas. • Not painful. • Spontaneous resolution occurs in 13-19% with residual scarring. • Treatment: potent topical steroids, intralesional steroids at the active border, or rarely systemic steroids
Granuloma Annulare (GA) • Controversy surrounds the association between GA and DM. • A case-control study by Nebesio et al. (5) failed to reveal a statistically significant correlation between the two. • A retrospective study by Studer et al. (6) suggested that up to 12% of patients presenting with GA had DM. • Despite conflicting studies, it is reasonable to screen patients presenting with GA for DM.
Granuloma Annulare (GA) • Appearance • Ring of small, firm, flesh-colored or red papules • If localized, most frequently found on lateral and dorsal surfaces of hands and feet • Disease begins with an asymptomatic, flesh-colored papule that undergoes central involution • Over months, a ring of papules grows • Can spontaneously regress without scarring • Histology • Focal degeneration of collagen in the upper and mid-dermis, palisaded histiocytes around collagen bundles, and abundant dermal mucin • Pathogenesis unknown
Granuloma Annulare (GA) • Treatment • If localized, best left untreated. • Can treat with intralesional steroids, if needed • If generalized, can also use dapsone, isotretinoin, freezing, cyclosporin, or PUVA.
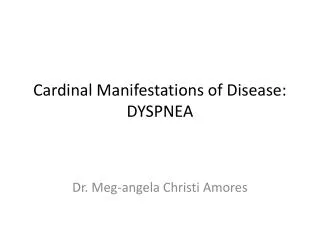
Granuloma Annulare (GA) Histology showing focal degeneration of collagen in the upper and mid-dermis, palisaded histiocytes around collagen bundles, and abundant dermal mucin
Diabetic Bullae • Approximately 0.5% of diabetics (2) • More common in men with long-standing DM and neuropathy • Two types have been described • More frequent, non-scarring lesions with a histologic intraepidermal split without acantholysis • Less common, occasionally hemorrhagic bullae that heal with scarring, slight atrophy, and have a histologic subepidermal split • Pathogenesis not well-understood • Could be related to trauma with reduced threshold for blister formation • Other theories include immunologic factors, disturbed catabolism of calcium, magnesium, or carbohydrates, microangiopathy, and vascular insufficiency • Appearance • Painless bullae on non-inflamed base that appear suddenly • Most common on the dorsa and sides of lower legs and feet, sometimes with similar lesions on the hands and forearms • Bullae contain clear, sterile fluid
Diabetic Bullae • Bullae tend to heal spontaneously in 2-5 weeks • Bullosis diabeticorum remains a diagnosis of exclusion with negative immunofluorescence studies, porphyrin levels, and cultures • DDx: bullous pemphigoid, epidermolysis bullosa acquisita, porphyria cutanea tarda, bullous impetigo, erythema multiforme, and coma blisters • May recur in the same or new locations • If large and symptomatic, can aspirate the fluid leaving an intact blister roof as a wound covering
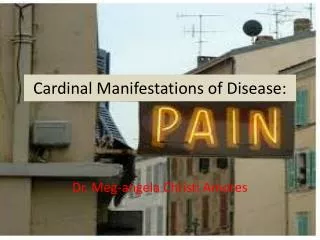
Histology showing a noninflammatory blister with a subepidermal and focally intraepidermal separation Diabetic Bullae
Acanthosis Nigricans • Seen in situations of insulin resistance • Besides in DM, also seen in the following: • Carcinomas, especially of the stomach • Secondary to meds (nicotinic acid, estrogen, or corticosteroids) • Pineal tumors • Other endocrine syndromes (PCOS, acromegaly, Cushing’s disease, hypothyroidism) • Obesity • Pathogenesis • According to Cruz (12) , it may be related to insulin binding insulin-like growth factor receptors on keratinocytes and dermal fibroblasts, thus stimulating growth.
Acanthosis Nigricans • Appearance • Hyperpigmented, velvety plaques in body folds, mostly axillae and neck • Can also present on groin, umbilicus, areolae, submammary areas, and on the hands (tripe hands) • Treatment- usually asymptomatic • Weight loss • Retinoic acid and salicylic acid
Skin Infections in DM • Occur in 20-50% of poorly controlled diabetics (2, 4) • More common in Type II • May be related to abnormal microcirculation, hypohidrosis, PVD, neuropathy, decreased phagocytosis and killing activity, impaired leukocyte adherence, and delayed chemotaxis all seen in diabetics (2, 9, 10, 11)
Skin Infections in DM • Fungal infections- most common • Candida • Candidal paronychia • Inframammary candida • Genital candida • Psedudohyphae and spores on KOH prep support dx of Candida • Purulent drainage may indicate secondary bacterial infection • Because maceration and skin breaks can serve as portals of infection, tinea pedis should be treated aggressively in diabetics • Treatment includes drainage of any abscesses, keeping the digits dry, and topical antifungals (clotrimazole)
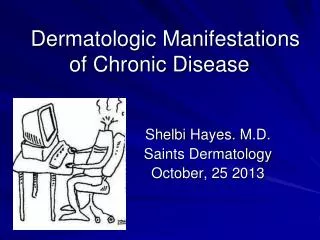
White, curdlike material adherent to erythematous, fissured oral commisure; angular stomatitis Candidiasis in Diabetics
Initial pustules on erythematous base that become eroded and confluent Candidiasis in Diabetics
Candidiasis in Diabetics KOH prep showing pseudohyphae and budding yeast forms
Skin Infections in DM • Bacterial Infections- can be more severe and widespread in diabetics • Malignant otitis externa • Pseudomonas aeruginosa • Fatal in over 50% patients (13) • Can progress to chondritis, osteomyelitis, and bacterial meningitis • Treat up to 3 months with oral quinolones but may need IV antibiotics
Skin Infections in DM • Bacterial infections in DM • Erythrasma • Reddish tan scaling patches of the upper inner thighs, axillae, toe web spaces, and inframammary creases • Gram positive Corynebacterium minutissimum • Identified with Wood’s light coral fluorescence • Treat with oral erythromycin for 5 days
Erythrasma in Diabetics • Reddish tan scaling patches of the upper inner thighs, axillae, toe web spaces, and inframammary creases
Cutaneous Manifestations of Diabetic Complications: Foot Ulcers • Responsible for 70% of annual lower limb amputations in the U.S.(2) • Large economic impact from medical and surgical therapy, rehab, loss of work, and mortality • Prevention is key • Daily foot inspections, appropriate footwear • Causes for ulcer formation: • Peripheral neuropathy (60-70%) • Treatment: aggressive debridement and offloading or with a contact cast • Vascular disease (15-20%) • Treatment: surgical re-vascularization • Combination of peripheral neuropathy and vascular disease (15-20%)
Cutaneous Reactions to Diabetic Treatment • Insulin • Allergy may be local or systemic and usually occurs within the first month of therapy • Erythematous or urticarial pruritic nodules at the site of injection • Lipoatrophy can also occur • Circumscribed depressed areas of skin at the insulin injection site 6-24 months after starting insulin • More common in women and children • Pathogenesis unknown but may be related to lipolytic components of the insulin preparation, an immune complex-mediated inflammatory process with lysosomal enzyme release, cryotrauma from refrigerated insulin, or mechanical trauma from injection • Lipohypertrophy can also occur • Soft dermal nodules that resemble lipomas at sites of frequent injection • May be a response to the lipogenic action of insulin • Treat and prevent by rotating sites of injection
Cutaneous Reactions to Diabetic Treatment- Insulin • Highly purified or recombinant insulins have a reduced allergy prevalence (0.1-0.2%) (4) • Observe the patient’s technique to make sure it isn’t intradermal • Treatment includes substitution of a more purified insulin, discontinuation or desensitization for severe systemic rxns