Download
1 / 20
270 likes | 2.43k Views
Testicular varicoceles. P. Beddy, et al. Clinical Radiology (2005) 60, 1248–1255. Type of study: review, but written as tutorial/editorial Aim: (not mentioned!! review of papers on varicocel Method of search: no methods mentioned. Varicocele.

E N D
Testicular varicoceles P. Beddy, et al. Clinical Radiology (2005) 60, 1248–1255
Type of study: review, but written as tutorial/editorial • Aim: (not mentioned!! review of papers on varicocel • Method of search: no methods mentioned
Varicocele • an abnormal venous dilatation in the pampiniform plexus • affects 15% of men • presentation: pain, swelling, sub-fertility • Most asympt
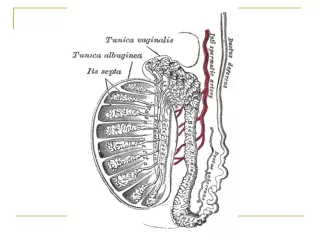
Etiology retrograde flow into internal spermatic vein dilatation/ tortuosity of the pampiniform plexus • Less frequent causes: • compression of renal vein (tumour) • aberrant renal vein • obstructed renal vein
Presentation • L>R (R.sp.v. enters obliquely into IVC: protective?) right side new in older R/O mass??
Diagnosis • clinical: if >3-4 mm (use valsalva) Amelar grading: • Grade 1: only palpable during Valsalva • Grade 2: palpable without the Valsalva • Grade 3: visible on examination
Imaging US • high-freq transducer (at least 7 MHz) • Sensitivity: 98% • Specificity: 100% Hamm et al. (1986): US in 118 patients, 2 mm was used as the lower limit for venous dilatation. • features on grey scale us: • at least 2-3 veins of the pampiniform plexus, • 1 vein diameter >2–3 mm in a supine position evidence: published study of 21 patients with clinically palpable varicoceles(ref: Rifkin et al. The role of diagnostic ultrasonography in varicocele evaluation. J Ultrasound Med 1983).
Diagnosis: Colour doppler • Evaluation in standing position (varicoceles to fill) • Diagnosis: detection of reverse flow in the incompetent vein • Reflux: • permanent (significant for a varicocele) • Intermittent • brief (physiological)
Diagnosis: doppler • sensitivity • 93% (n=14 pts.; Petros et al. 1991) • clinic exam sensitivity: 71%
Diagnosis: venography • Gold standards • normal venogram: • a single testicular vein is seen up to the inguinal ligament and into the spermatic cord • Varicocele: • enlarged int spermatic vein • reflux into abdominal, inguinal, scrotal or pelvic portions of the spermatic vein
Diagnosis: MRI (MRV) • gadolinium-enhanced imaging • delayed imaging in venous • dilated vessels and prominence of the pampiniform plexus • indication • evaluate the presence of obstructing masses • Conventional venography is contraindicated • assessment of recurrent varicoceles.
Treatment • symptomatic • subfertility • percutaneous embolization (choice) • surgical (failed catheterization) • Recurrence rate: similar • randomised, prospective study. Barbalias et al. 1998
Percutaneous embolization • Selective catheterization of the spermatic vein • embolization with a sclerosing agent or a solid coil
Coil: distal: the level of inguinal lig. prox: 2–3 mm of renal vein • all collateral veins occluded
Sclerosing agents • such as sodium tetradecyl sulphate • reflux into pampiniform plexus is prevented by external pressure
Radiological Rx • success rate > 90% • Failure: due to unsuccessful catheterization or anatomical variants
Good • Easy to read • General overview of clinical dx+Rx • Nice pictures with appropriate titles/legends
Bad • No method of review • emphasis on personal practice without research evidence back up