Download
1 / 33
340 likes | 415 Views
Testicular carcinoma affects mostly white males aged 15-35 and is usually a germ cell tumor. Learn about risk factors, clinical manifestations, and diagnosis methods such as U/S, CXR, and markers like AFP and B-HCG. Treatment principles include radiotherapy for seminomas and surgery for non-seminomas. Explore different subtypes like seminoma, embryonal, yolk sac, choriocarcinoma, and teratoma. Understanding TNM staging and the importance of early detection and treatment.

E N D
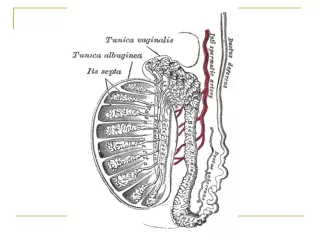
Epidemilogy • 90-95% are germ cell • Incidence five times higher among white men • Most common solid tumor in males ages 15-35 • often is in right
What is Testicular Cancer? • Germ cell tumors (GCT): ~95% of TC • Seminomas: most common subtype (~50%); slow growing and radiosensitive • Nonseminomas: often occur in third decade; rapid metastasis to lymph nodes and lung • Non-Germ Cell Tumors (Non-GCTs) • Stromal: ~4% of adult TC • Secondary tumors: arise in another organ
Risk factor • Gonadal Dysgenesis • 20-30% develop cancer (gonadoblastoma) • Trauma • prompts evaluation • Hormones • DES/OCP probably do not increase risk • Atrophy (mumps orchitis)
Cryptorchidism: 7-10% of patients with testicular cancer have a history of cryptorchidism • Abnormal germ cell morphology • Elevated temperature • Interference with normal blood supply • 5-10% of patients with testicular cancer and a history of cryptorchidism develop cancer in the contralateral testis • Orchidopexy does not prevent development of cancer – just allows for detection
Clinical manifestation • Patients often present with a painless testicular mass • Pain, swelling, or hardness in scrotum a less frequent complaint • About 10% report recent testicular trauma • Swelling in lower extremities, back pain, cough, or dyspnea may indicate advanced disease • Gynecomastia • 5% germ cell • 30-50% Sertoli/Leydig • 1-2% have bilateral disease at diagnosis • More common on the right
Diffrentiated Diagnosis • Torsion • Epididymitis • Epididimoorchitis • Hydrocele • Hernia • Hematoma • Spermatocele • Syphilitic gumma
Work-up • Exam • U/S • CXR +/- Chest CT • Abdominal CT • Can identify small nodal deposits <2 cm • MRI and PET scan no advantage over CT • Markers • Elevation after orchiectomy generally represents metastatic disease • Conversely normalization does not rule out metastatic disease
Alpha-Fetoprotein • Expressed by the early embryo (also liver and GI tract) • Single chain • Half-life: 5-7 days • Produced by pure embryonal, teratocarcinoma, yolk sac, mixed tumors (NOT pure choriocarcinoma or seminoma) • Falsely elevated in liver dysfunction, viral hepatitis
Human Chorionic Gonadotrophin • Secretory product of the placenta • Alpha unit (LH,FSH,TSH) and beta unit • Half-life: 24-36 hours • Produced by syncytiotrophoblastic tissue • All choriocarcinomas, 40-60% embryonal, 5-10% seminoma • Falsely elevated in hypogonadism and marijuana use
Lactic Acid Dehydrogenase • Presents normally in smooth, cardiac and skeletal muscle, liver and brain • Most useful in advanced seminoma or tumors where other markers are not elevated • Many false positives
Testis cancer GERM CELL • Seminoma 30-60% • Non-seminoma Embryonal 3-4% Yolk sac Teratoma 5-10% Choriocarcinoma 1% Mixed 40% NONGERM CELL • Leydig 1-3% • Sertoli <1% • Gonadoblastoma 0.5%
Seminoma: • Most common germ cell tumor • Pure seminomas never secrete AFP • 5-10% secrete HCG (usually classic) • At diagnosis: • 65-75% confined to the testis • 10-15% with regional retroperitoneal nodes • 5-10% with advanced juxtorenal or visceral disease
Classic 82-85% • Age 30s • Islands /sheets of cells with syncytiotrophoblasts (5-10%) • Anaplastic 5-10% • Stage for stage no different than classic • Spermatocytic 2-12% • Low metastatic potential • Older population (>50) • 6% bilateral
Emberional • Peak age 25-35 • May secrete both AFP and B-HCG • Metastatic deposits usually contain teratoma (80%)
Yolk Sac (Infantile embryonal) • Peak age: infants and children • Also may spread hematogenously • Secretes AFB and B-HCG • Embryoid bodies (Schiller-Duvall bodies) resemble 1-2 week old embryos surrounded by syncytiotrophoblasts and cytotrophoblasts
Choriocarcinoma • Peak age 20-30 • Worst prognosis of all testis tumors • Hematogenous spread (especially to lungs) • Always secrete B-HCG
Teratoma • Peak age 25-35 • Poor response to chemotherapy and XRT • Pure forms should not secrete AFB or B-HCG • Can arise from malignant transformation after chemotherapy for NSGCT • Contains all 3 germ layers in the mature form and is undifferentiated in immature form
TNM Staging of Testicular Tumour • T0 = No evidence of Tumour • T1s = Intratubular, pre invasive • T1 = Confined to Testis • T2 = Invades beyond Tunica Albuginea or into • Epididymis • T3 = Invades Spermatic Cord • T4 = Invades Scrotum • N1 = Multiple< 5 node/Single < 2 cm • N2 = Multiple < 5 node / Single 2-5 cm • N3 = Any node > 5 cm
PRINCIPLES OF TREATMENT • Treatment should be aimed at one stage above the clinical stage • Seminomas - Radio-Sensitive. Treat with Radiotherapy. • Non-Seminomas are Radio-Resistant and best treated by Surgery • Advanced Disease or Metastasis - Responds well to Chemotherapy
PRINCIPLES OF TREATMENT • Radical INGUINAL ORCHIDECTOMY is Standard first line of therapy • Lymphatic spread initially goes to RETRO-PERITONEAL NODES • Early hematogenous spread RARE • Bulky Retroperitoneal Tumours or Metastatic Tumors Initially “DOWN-STAGED” with CHEMOTHERAPY
Treatment of Seminomas Stage I, IIA- Radical Inguinal Orichidectomy followed by radiotherapy to Ipsilateral Retroperitonium & Ipsilateral Iliac group Lymph nodes (2500-3500 rads) Bulky stage II and III Seminomas - Radical Inguinal Orchidectomy is followed by Chemotherapy
Treatment of Non-Seminoma Low Grade RADICAL ORCHIDECTOMY followed by RETROPERITONEAL LYMPH DISSECTION High Grade: Initial CHEMOTHERAPY followed by SURGERY for Residual Disease
NON_GERM CELL Leydig Cell • 1-3% of all testis tumors • Bimodal age distribution: ages 5-9 and 25-35 • Bilateral in 5-10% • No association with cryptorchidism • Prepubital children may present with virilization and elevated urinary 17-ketosteroid levels; adults are usually asymptomatic (25% gynecomastia) • Treatment: radical orchiectomy and RPLND for malignant tumors (10% malignant)
Sertoli Cell • Less than 1% of all testicular tumors • Bimodal age of distribution: < 1 year and 20-45 years old • 10% lesions are malignant • Virilization seen in children and gynecomastia in adults • Treatment: Radical orchiectomy with RPLND in malignant disease
Gonadoblastoma • 0.5% of testicular tumors • Seen in patients with gonadal dysgenesis • 4/5 patients are phenotypic females with streak gonads • Treatment: Radical orchiectomy with gonadectomy of the contralateral gonad (bilateral in 50%)
Secondary testicular tumor • Lymphoma Large without pain 50% bilatral ¼ with systemic symptom treatment: radical orciectomy+chemotherapy
Leukemia: in 50% bilatral Dx : biopsy • Metastatic tumor: very rarely source: prostat lung GI melanoma kidney