Download
1 / 30
380 likes | 1.21k Views
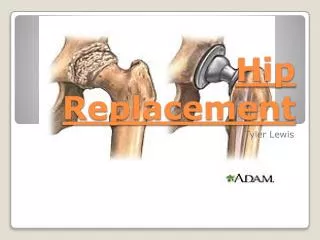
TOTAL HIP REPLACEMENT. Presented by: Atillio Castellani Brendan Cochren Trevor Kelly Shuntaro Maruyama Mustafa Sharif. General Anatomical Overview. The hip is one of your body's largest weight-bearing joints. Consists of two main parts:

E N D
TOTAL HIP REPLACEMENT Presented by: Atillio Castellani Brendan Cochren Trevor Kelly Shuntaro Maruyama Mustafa Sharif
General Anatomical Overview • The hip is one of your body's largest weight-bearing joints. • Consists of two main parts: • a ball (femoral head) that fits into a rounded socket (acetabulum) in your pelvis. • Ligaments connect the ball to the socket and provide stability to the joint • The bone surfaces of your ball and socket have a smooth durable cover of articular cartilage that cushions the ends of the bones and enables them to move easily.
More… • All remaining surfaces of the hip joint are covered by a thin, smooth tissue called synovial membrane. In a healthy hip, this membrane makes a small amount of fluid that lubricates and almost eliminates friction in your hip joint. • Normally, all of these parts of your hip work in harmony, allowing you to move easily and without pain.
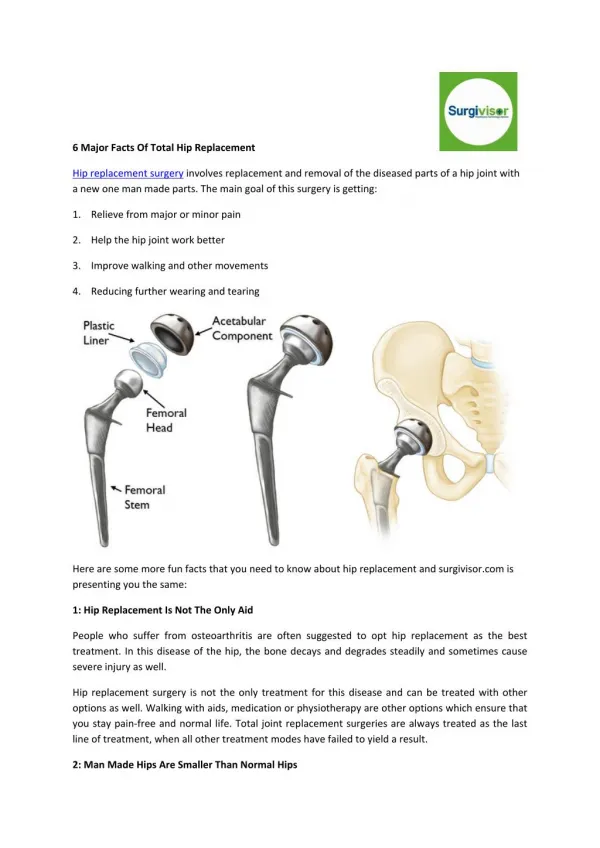
Total Hip Replacement • A prosthetic hip that is implanted in a similar fashion as is done in people. It replaces the painful arthritic joint. • The modular prosthetic hip replacement system used today has three components – the femoral stem, the femoral head, and the acetabulum. Each component has multiple sizes which allow for a custom fit. • The components are made of cobalt chrome stainless steel and ultra high molecular weight polyethylene. Cementless and cemented prosthesis systems are available.
Statistical Overview • First performed in 1960. • Since then, improvements in joint replacement surgical techniques and technology have greatly increased the effectiveness of this surgery.
Number of Total Hip and Total Knee Replacement Procedures Performed in Canada, 1994–1995 to 2001–2002
Number and Distribution of Total Hip Replacement Procedures by Age Group and Sex, Canada, 2001–2002 Compared to 1994–1995 Source: Hospital Morbidity Database, CIHI
Subjective Assessment • Pain localized in hip region • Exaggerated gait pattern (limp) • Increase in pain when weight barring • Reduction in the degree of ROM • As the degeneration of the joint worsen, individual may be awakened at night with pain • Bone spurs may occur
Objective Assessment • Gait pattern – Adaptive walking pattern that reduces pressure on the affected side. • Muscle atrophy – Muscles in affected area are not used as much due to pain, therefore, use-it-or-lose-it applies. • Active Range Of Motion – Limited ROM, stiffness • Passive ROM – End feels causes severe pain • X-ray – clear degeneration of the bone • MRI – determines underlying complications (e.g.avascular necrosis)
Common Causes of Hip Pain and Loss of Hip Mobility Osteoarthritis • Usually occurs after age 50 and often in an individual with a family history of arthritis. In this form of the disease, the articular cartilage cushioning the bones of the hip wears away. The bones then rub against each other, causing hip pain and stiffness.
Causes (cont’d) Rheumatoid Arthritis • a disease in which the synovial membrane becomes inflamed, produces excessive synovial fluid, and damages the articular cartilage, leading to pain and stiffness.
Causes (cont’d) Traumatic Arthritis • Can leads to a serious hip injury or fracture. A hip fracture can cause a condition known as avascular necrosis. The articular cartilage becomes damaged and, over time, causes hip pain and stiffness.
Osteoarthritis Fracture
OperationRemoving the Femoral Head • Once the hip joint is entered, the femoral head is dislocated from the acetabulum. • Then the femoral head is removed by cutting through the femoral neck with a power saw.
Reaming the Acetabulum • After the femoral head is removed, the cartilage is removed from the acetabulum using a power drill and a special reamer. • The reamer forms the bone in a hemispherical shape to exactly fit the metal shell of the acetabular component.
Inserting the Acetabular Component • A trial component, which is an exact duplicate of your hip prosthesis, is used to ensure that the joint will be the right size and fit for the client. • Once the right size and shape is determined for the acetabulum, the acetabular component is inserted into place.
Preparing the Femoral Canal • To begin replacing the femoral head, special rasps are used to shape and scrape out femur to the exact shape of the metal stem of the femoral component. • Once again, a trial component is used to ensure the correct size and shape. The surgeon will also test the movement of the hip joint.
Inserting Femoral Stem • Once the size and shape of the canal exactly fit the femoral component, the stem is inserted into the femoral canal.
Attaching the Femoral Head • The metal ball that replaces the femoral head is attached to the femoral stem.
The Completed Hip Replacement • Client now has a new weight bearing surface to replace the affected hip. • Before the incision is closed, an x-ray is made to ensure new prosthesis is in the correct position.
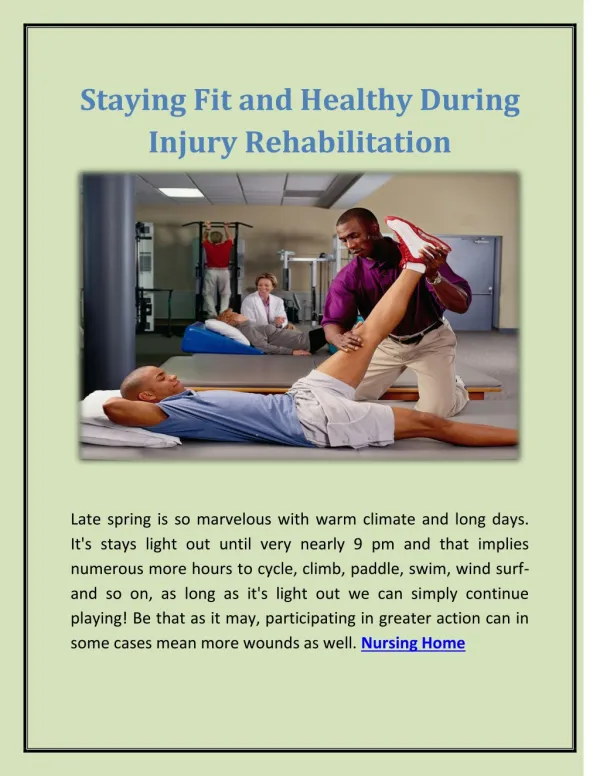
Treatment by Kinesiologist-Early Postoperative Exercises- • Regular exercises to restore your normal hip motion and strength and a gradual return to everyday activties. • Exercise 20 to 30 minutes a day divided into 3 sections. • Increase circulation to the legs and feet to prevent blood clots • Strengthen muscles • Improve hip movement
Kinesiologist’s Role (cont) • The patient is released few days after the surgery • A list of Do’s and Don’ts • Hip is sore and weak • Start with light exercises • Ergonomics: Rearrange furniture in the house to make using crutches easier. Setup a ‘recovery centre’, a table where u put phone, remote control, radio, medication and other essential things that you need. It makes it more accessible.
Educate Clients- Do’s and Don’ts - • To avoid hip dislocation: • Using 2-3 pillows between your legs when sleeping (roll onto your ‘good side’ • Not crossing your legs • Use chairs with armrest • Not bending forward past 90 degrees • Using a high-rise toilet seat if necessary • Avoid pronation the legs • To avoid stairs, sleep in the living room
Post-Surgery Complications • Thrombophlebitis • the blood in the large veins of the leg forms blood clots within the veins. • If the blood clots in the veins break apart they can travel to the lung. • Infection in the joint • Dislocation of the joint • Loosening of the joint
3 QUESTIONS 1. What are the two structures involved in the total hip replacement surgery? a) head of femur (ball) b) acetabulum (socket) c) greater trochanter (femur) d) Ischial tuberosity Answer: a & b 2. Which of the following (s) could lead to a total hip replacement? a) high blood pressure b) rheumatoid arthritis c) hip fracture d) all of the above Answer: b & c 3. Which of the following (s) is a possible post-surgery complication for a total hip replacement? a) thrombophlebitis b) infection in joint c) dislocation of joint d) all of the above Answer: d
Reference • Unversity of Iowa Hospitals and Clinics. (January 2005). Total Hip Replacement: A Guide for Patient. Retrieved on Novemember 20th 2005, from http://www.vh.org/adult/patient/orthopaedics/hipreplace/ • American Academy of Orthopedic Surgeons. (June 2001). Total Hip Replacement. Retrieved on November 20th 2005, from http://orthoinfo.aaos.org/booklet/view_report.cfm?thread_id=2&topcategory=Hip • MedicineNet.com. (October 2005). Total Hip Replacement. Retrieved on November 20th 2005, from http://www.medicinenet.com/total_hip_replacement/article.htm • Gulf Coast Veterinary Specialists. (2002). Total Hip Replacement. Retrived on November 20th 2005, from http://www.gcvs.com/surgery/total_hip.htm • Medical Multimedia Group. (May 17th 1997). A Patient’s Guide to Total Hip Replacement Surgery. Retrieved on November 20th 2005, from http://www.healthpages.org/AHP/LIBRARY/HLTHTOP/THR/INDEX.HTM • Canadian Institute of Health Information. (March 31st 2004). More than 10% of Total Hip Replacements are for Repeat Surgeries, Reports Canadian Institute for Health Information (CIHI). Retrieved on November 21st 2005, from http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=media_09oct2002_e