Download
1 / 11
110 likes | 667 Views
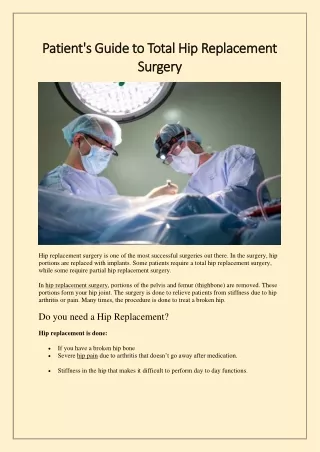
Total Hip Replacement. Dr. Belal Hijji, RN, PhD March 21, 2012. Learning Outcomes. At the end of this lecture, students will be able to Define total hip replacement and identify its indications.

E N D
Total Hip Replacement Dr. Belal Hijji, RN, PhD March 21, 2012
Learning Outcomes At the end of this lecture, students will be able to • Define total hip replacement and identify its indications. • Discuss the nursing interventions designed to prevent complications following total hip replacement. • Describe the content of teaching that should target the patient postoperatively.
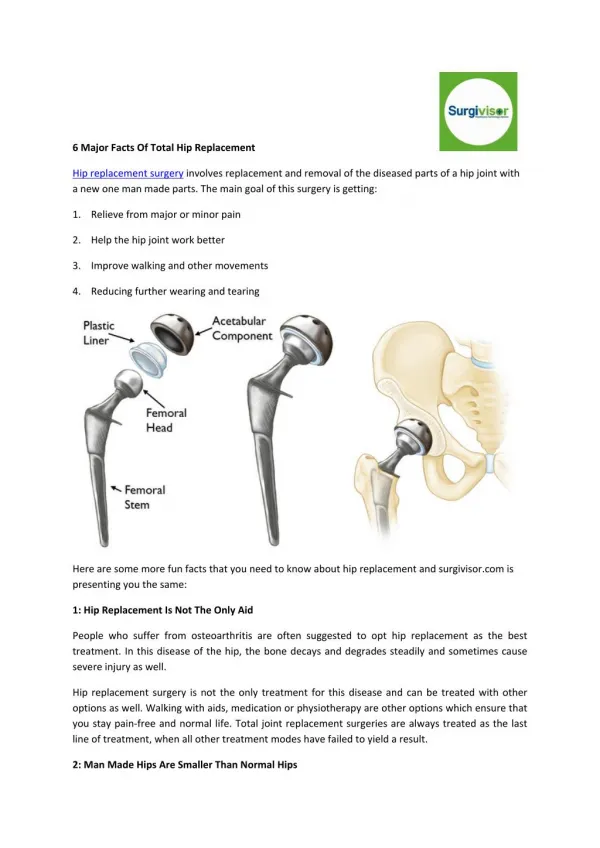
Definition of, and indications for, Total Hip Replacement • Total hip replacement is the replacement of a severely damaged hip with an artificial joint. • This surgical procedure is indicated in several conditions including rheumatoid arthritis, femoral neck fractures, and failure of previous reconstructive surgeries (failed prosthesis). • Most total hip prostheses consist of a metal femoral component topped by a spherical ball fitted into a plastic acetabular socket (see Figure). The surgeon selects the prosthesis that is most suited to the individual patient.
Nursing interventions • The nurse must be aware of and monitor for specific potential complications including dislocation of the hip prosthesis, excessive wound drainage, thromboembolism, infection, and heel pressure ulcer. Other complications are those associated with immobility, formation of bone in the periprosthetic space, bone death caused by loss of blood supply, and loosening of the prosthesis.
Preventing Dislocation of The Hip Prosthesis • The nurse teaches the patient about positioning the leg in abduction by using two or three pillows between the legs, which helps to prevent dislocation of the prosthesis. • When the nurse turns the patient in bed, it is important to keep the operative hip in abduction. • The patient’s hip is never flexed > 90°. To prevent hip flexion, the nurse does not elevate the head of the bed more than 60°. For using a bedpan, the nurse instructs the patient to flex the unaffected hip and to use the trapeze (slide 6) to lift the pelvis onto the pan. • The nurse teaches the patient about maintaining abduction and avoiding internal and external rotation, hyperextension, and acute flexion. • The patient should not sleep on the affected side without consulting the surgeon, and no crossing of the legs.
Slip the bedpan under the patient’s buttocks while she lifts herself with the trapeze
Monitoring Wound Drainage • Postoperatively, fluid and blood accumulating at the surgical site are removed (200 to 500ml in the first 24 hours). After 48 hours postoperatively, the total drainage in 8 hours decreases to 30 mL or less, and the suction device is then removed. • The nurse promptly reports any drainage volumes greater than anticipated.
Preventing Deep Vein Thrombosis • The incidence of DVT, which occurs 5-7 day postoperatively, is 45% to 70%. About 20% of patients with DVT develop pulmonary embolism , of which about 1% to 3% of cases are fatal. • The nurse monitors the patient closely for signs and symptoms of DVT (calf pain, swelling, and tenderness). • The nurse encourages the patient to take enough fluids, to perform ankle and foot exercises hourly while awake, to use elastic stockings as prescribed, and to transfer out of bed and ambulate with assistance beginning on the first postoperative day. Low-dose heparin is frequently prescribed as prophylaxis for DVT after hip replacement surgery.
Preventing Infection • Infection, a serious complication of total hip replacement, may necessitate removal of the implant. Patients at high risk of developing infection include the elderly, obese, or poorly nourished. Others those who have diabetes, rheumatoid arthritis, urinary tract infection, and dental abscess. • The nurse administers prophylactic antibiotics as prescribed. • Used indwelling urinary catheters or portable wound suction devices are removed sooner to avoid infection.
Teaching the Patient Self-Care • Before discharge, the nurse advises the patient of the importance of the daily exercise program to maintain the functional motion of the hip joint and strengthening the abductor muscles (slide 11), and reminds the patientthat it will take time to strengthen and retrain the muscles. • Assistive devices (crutches, walker, or cane [عصا]) are used, until normal gait without discomfort is pursued (3 months). • The patient may need assistance in putting on shoes and socks. • The patient should avoid low chairs and sitting for longer than 45 minutes at a time to minimize hip flexion and the risks for prosthetic dislocation, hip stiffness, and flexion contracture (The patient is unable to fully straighten his leg either actively or passively).