Download
1 / 23
330 likes | 1.8k Views
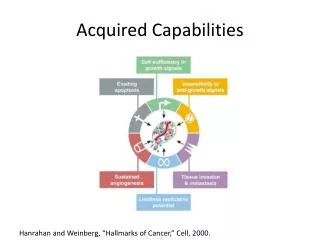
30 August 2011. 2. ICU-acquired Weakness. ExamplesCase studyIncidence rateRisk factorsCurrent understandingPractical implications. 30 August 2011. 3. 30 August 2011. 4. 30 August 2011. 5. 30 August 2011. 6. . 30 August 2011. 7. 30 August 2011. 8. Ms. KK. 59F c Ao stenosis, sm bowel AVMsPMH: DM, HTN, dyslipidemia, CADLaparoscopic LOADouble-balloon enteroscopy.

E N D
1. 30 August 2011 ICU-acquired Weakness Ronald Jou
2. 30 August 2011 2 ICU-acquired Weakness Examples
Case study
Incidence rate
Risk factors
Current understanding
Practical implications Some pictures first.Some pictures first.
3. 30 August 2011 3
4. 30 August 2011 4
5. 30 August 2011 5
6. 30 August 2011 6
7. 30 August 2011 7
8. 30 August 2011 8 Ms. KK 59F c Ao stenosis, sm bowel AVMs
PMH: DM, HTN, dyslipidemia, CAD
Laparoscopic LOA
Double-balloon enteroscopy
9. 30 August 2011 9 Ms. KK POD #2: abd pain and distension
EX LAP: two enterotomies
ICU admission
Severe sepsis
Adrenal insufficiency POD #2: abd pain, distension
EX LAP: two enterotomies found and repaired
ICU admission
Severe sepsis
PA catheter
Pressors
Broad spectrum abx
Adrenal insufficiency
POD #2: abd pain, distension
EX LAP: two enterotomies found and repaired
ICU admission
Severe sepsis
PA catheter
Pressors
Broad spectrum abx
Adrenal insufficiency
10. 30 August 2011 10 Ms. KK Sepsis resolved
Prolonged mechanical ventilation
ICU #14
Sedation discontinued
Patient unable to move arms or legs
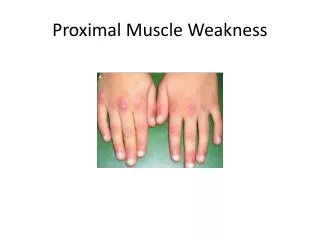
She had 1/5 weakness proximally and 0/5 weakness distally.
We were concerned about neuropathy/myopathy of critical illness.
Neurology consultation: Exam was confirmed and EMG showed polyneuropathy with impaired motor and sensory conduction.She had 1/5 weakness proximally and 0/5 weakness distally.
We were concerned about neuropathy/myopathy of critical illness.
Neurology consultation: Exam was confirmed and EMG showed polyneuropathy with impaired motor and sensory conduction.
11. 30 August 2011 11 Early Observations MacFarlane, et al. Severe myopathy after status asthmaticus. Lancet. 1977.
Zochodne, et al. Critical illness polyneuropathy. Brain. 1987. MacFarlane: Small series of patients. All treated with hydrocortisone. Sedation with a combination of midazolam and pancuronium infusion.
Zochodne: Canada. 19 patients with sepsis, MOD. One month ventilator durations. Weakness, muscle wasting, impaired DTRs, abnormal electrophysiological studies. �[The study] failed to reveal putative metabolic, drug, nutritional or toxic factors that might be responsible for the polyneuropathy.�MacFarlane: Small series of patients. All treated with hydrocortisone. Sedation with a combination of midazolam and pancuronium infusion.
Zochodne: Canada. 19 patients with sepsis, MOD. One month ventilator durations. Weakness, muscle wasting, impaired DTRs, abnormal electrophysiological studies. �[The study] failed to reveal putative metabolic, drug, nutritional or toxic factors that might be responsible for the polyneuropathy.�
12. 30 August 2011 12 Differential Diagnosis Spinal cord injury
Amyotrophic lateral sclerosis
West Nile virus
Chronic myelopathy
Myasthenia gravis
Rhabdomyolysis
Hypo K+/phos Spinal cord: trauma,
ALS usually chronic
West Nile is rare
Chronic myelopathy: toxins, porphyria, cord-compression, vasculitis
MG
Muscle dystrophySpinal cord: trauma,
ALS usually chronic
West Nile is rare
Chronic myelopathy: toxins, porphyria, cord-compression, vasculitis
MG
Muscle dystrophy
13. 30 August 2011 13 ICU-acquired Weakness
14. 30 August 2011 14 Clinical Syndrome Acquired during critical illness
Tetraparesis
Impaired DTRs
Ventilator dependence
Abnormal electrophysiologic studies
Abnormal histologic examination In other words: when should you suspect this?
Electrophysiologic studies: EMG (electromyography), sensory nerve conduction study, direct muscle stimulation.In other words: when should you suspect this?
Electrophysiologic studies: EMG (electromyography), sensory nerve conduction study, direct muscle stimulation.
15. 30 August 2011 15 Studies Population
Observational
Risk factors
Natural history Clinical testing requires awake, cooperative patient.
Not well-defined (clinical v. electrophys v. histopath)Clinical testing requires awake, cooperative patient.
Not well-defined (clinical v. electrophys v. histopath)
16. 30 August 2011 16 Incidence Rate ~2% of mechanically ventilated patients
~10% of mechanical ventilation ? 7 days
~60-85% of patients with severe sepsis
17. 30 August 2011 17 Risk Factors? SIRS, sepsis, APACHE score, NMBA, steroids, aminoglycoside therapy, renal replacement, TPN, furosemide?SIRS, sepsis, APACHE score, NMBA, steroids, aminoglycoside therapy, renal replacement, TPN, furosemide?
18. 30 August 2011 18 Pathogenesis? UMN lesion: encephalopathy is common in critical illness. Sepsis alone can cause encephalopathy in absence of end-organ dysfunction.
SIRS, TNF-?, IL-1, all cause disruption of microcirculation, leading to local immune activation, endoneural edema, and local hypoxia.
NMJ: Pharmacokinetics of prolonged NMBA infusion, active metabolites, potentiated by aminoglycosides, decreased clearance in renal failure.
Myopathy: Steroids.
UMN lesion: encephalopathy is common in critical illness. Sepsis alone can cause encephalopathy in absence of end-organ dysfunction.
SIRS, TNF-?, IL-1, all cause disruption of microcirculation, leading to local immune activation, endoneural edema, and local hypoxia.
NMJ: Pharmacokinetics of prolonged NMBA infusion, active metabolites, potentiated by aminoglycosides, decreased clearance in renal failure.
Myopathy: Steroids.
19. 30 August 2011 19 ICU-acquired Weakness
20. 30 August 2011 20 Practical Implications Common
May not be avoidable
Prolongs critical illness
Clinical suspicion
Treatment?
Prognosis? Garnacho (Seville, Spain): Length of mechanical ventilation 34 d v. 14 d (p < 0.001) and duration of weaning 15 d v. 2 d (p < 0.001).Garnacho (Seville, Spain): Length of mechanical ventilation 34 d v. 14 d (p < 0.001) and duration of weaning 15 d v. 2 d (p < 0.001).
21. 30 August 2011 21 Ms. KK Revisited Severe sepsis
NMBA
Steroids
Strength improved to 2/5
Extubated ICU #18
Transferred to ward ICU #22
22. 30 August 2011 22 References De Jonghe B, Cook D, Sharshar T, Lefaucheur JP, Carlet J, Outin H. Acquired neuromuscular disorders in critically ill patients: a systematic review. Groupe de Reflexion et d'Etude sur les Neuromyopathies En Reanimation. Intensive Care Med 1998;24(12):1242-50.
De Jonghe B, Sharshar T, Lefaucheur JP, et al. Paresis acquired in the intensive care unit: a prospective multicenter study. Jama 2002;288(22):2859-67.
de Letter MA, Schmitz PI, Visser LH, et al. Risk factors for the development of polyneuropathy and myopathy in critically ill patients. Crit Care Med 2001;29(12):2281-6.
De Letter MA, van Doorn PA, Savelkoul HF, et al. Critical illness polyneuropathy and myopathy (CIPNM): evidence for local immune activation by cytokine-expression in the muscle tissue. J Neuroimmunol 2000;106(1-2):206-13.
Deem S. Intensive-care-unit-acquired muscle weakness. Respir Care 2006;51(9):1042-52; discussion 52-3.
Garnacho-Montero J, Amaya-Villar R, Garcia-Garmendia JL, Madrazo-Osuna J, Ortiz-Leyba C. Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients. Crit Care Med 2005;33(2):349-54.
Garnacho-Montero J, Madrazo-Osuna J, Garcia-Garmendia JL, et al. Critical illness polyneuropathy: risk factors and clinical consequences. A cohort study in septic patients. Intensive Care Med 2001;27(8):1288-96.
23. 30 August 2011 23