Download
1 / 35
370 likes | 788 Views
Acute Peripheral Weakness. Peter Shearer, MD Assistant Residency Director Mt. Sinai School of Medicine. Objectives. Acute Extremity Weakness Levels of potential involvement Key Elements of History and Physical for each level CNS PNS Diagnostic Options Therapy. Question #1.

E N D
Acute Peripheral Weakness Peter Shearer, MDAssistant Residency DirectorMt. Sinai School of Medicine
Objectives • Acute Extremity Weakness • Levels of potential involvement • Key Elements of History and Physical for each level • CNS • PNS • Diagnostic Options • Therapy
Question #1 At which level of the CNS can a lesion produce motor weakness without affecting mental status? A. Brainstem B. Dorsal root ganglia C. Spinal Cord D. Cerebellum
Question #2 Which of the following can differentiate between acute transverse myelitis and Guillain-Barre Syndrome? A. ascending vs. descending paralysis B. presence of slight lymphocytosis in CSF C. increased vs. decreased reflexes D. acuity of onset E. presence of a preceding respiratory or GI illness
Question #3 Which of the following does NOT produce a myelopathy? A. Spinal cord infarct B. Transverse Myelitis C. Spinal cord metastasis of lung cancer D. Tick Paralysis
Question #4 Which of the following illnesses has a well evaluated, prospectively studied therapy? A. Guillain-Barre Syndrome B. Acute Transverse Myelitis C. Acute Spinal Cord Hemorrhage D. Botulism
case-history • 30 year old woman • diffuse weakness • lower extremities > upper extremities • over 3 days • preceding diffuse vesicular rash • difficulty voiding
case-history • 30 year old woman • diffuse weakness • lower extremities > upper extremities ascending • over 3 days • preceding diffuse vesicular rash • difficulty voiding
case-details of the physical • BP 140/86, P 90, RR 18, T 99, 99%O2 sat • CN intact • Motor: 4/5 in UE, 3/5 in LE • Sensory intact but sharp/dull less pronounced in the LE • Reflexes 3+ in all extremities • palpable bladder
Case - summary • Acute ascending symmetrical paralysis following a recent infection with slight sensory impairment and hyperreflexia.
Could this be a CNS lesion? Yes Can a CNS lesion produce bilateral weakness and sensory deficits and have a normal mental status?
Could this be a CNS lesion? • CNS = Upper motor neuron • cerebral cortex to, but not including the anterior horn cell • UMN lesions produce: • increased tone • increased DTR • extensor plantars • no fasiculations
levels of the CNS • Cerebral Cortex • Cerebellum • Brainstem • Spinal Cord up to the Anterior Horn Cell
Could this be a PNS lesion? Yes Where?
levels of the PNS • Spinal cord - Anterior horn cell of the Lateral Corticospinal tract • Peripheral nerve • NMJ • Muscle
Myelopathy • A Lesion in the cord produces A Level of deficit • Division of labor • Dorsal columns - position/vibration • Lateral corticospinal tract - motor function • Lateral spinothalamic tract - pain/temperature • Preserved mental status
Myelopathy - etiology • Infarct • Trauma • Brown-Sequard • Central cord syndrome • Anterior cord syndrome • Mass lesions • Inflammation/Infection
myelopathy - details of history • Acuity of onset • Trauma • Distal > Proximal • Pain at site • Preceding Illness
myelopathy - details of physical • Weakness • Spasticity • Atrophy • Fasciculations • Bowel and bladder complaints • Increased tone • Sensory findings • DTR’s may be increased (not if ALS)
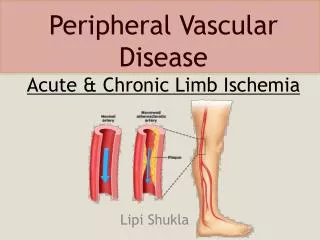
Cord Infarct • Anterior Spinal Artery • anterior cord - dissociation of sensory findings • symmetric flaccid paralysis • loss of sphincter tone • Dorsal columns prevail • Posterior Spinal Artery • proprioceptive and vibratory sensation
Acute Peripheral Neuropathy • Motor and/or sensory • disorder of transmission along peripheral nerve • axon • myelin • Guillain-Barre • Tick Paralysis • Toxic
Acute Peripheral Neuropathy - details of physical • Weakness • Absent DTR’s (all outflow from the cord is affected) • Affects longer nerves first - ascending
Guillain-Barre Syndrome • Post infectious • mononuclear inflammatory infiltrate of myelin • dymyelinating • may be axonal injury and degeneration
Guillain-Barre Syndrome • Symmetric ascending paralysis • areflexic • possible sensory - paresthesias, position and vibration • Progression over 1 - 3 weeks - may be more rapid • 1/3 progress to respiratory failure
Guillain-Barre Syndrome • CSF - Albuminocytologic dissociation • Stool for C. jejuni
NMJ • Presynaptic - disorder of ACh release • will affect nicotinic and muscarinic • weakness • anticholinergic symptoms • Postsynaptic - will just be nicotinic • weakness • NO anticholinergic findings
NMJ - details of history • Exposure • botulism • snake bites • fatigue
NMJ - details of physical • Proximal>distal muscles • Bulbar muscles • May have anticholinergic signs if presynamptic • Fatigability
Examples of NMJ disorders • Myasthenia Gravis • Botulism • Tick Paralysis
Myopathies • Periodic Paralyses • Electrolyte Abnormalities • Hypermagesemia • Hypophosphatemia
Metabolic Abnormalities • Periodic Paralyses • Hypermagesemia • Hypophosphatemia
Work up • CBC and serum chemistry • CSF for signs of GBS or myelitis • Radiography • MRI vs CT
Management • Corticosteroids • not supported by prospective placebo controlled studies