Download
1 / 87
880 likes | 1.07k Views
Volume 361:1088-1097 September 10, 2009 Number 11 Parenteral Nutrition in the Critically Ill Patient Thomas R. Ziegler, M.D. .

E N D
Volume 361:1088-1097September 10, 2009Number 11 Parenteral Nutrition in the Critically Ill Patient Thomas R. Ziegler, M.D.
A 67-year-old woman with type 2 diabetes mellitus undergoes extensive resection of the small bowel and right colon with a jejunostomy and colostomy because of mesenteric ischemia. In the surgical intensive care unit, severe systemic inflammatory response syndrome with possible sepsis develops. The patient is treated with volume resuscitation, vasopressor support, mechanical ventilation, broad-spectrum antibiotics, and intravenous insulin infusion.
Low-dose tube feedings are initiated postoperatively through a nasogastric tube. However, these feedings are discontinued after the development of escalating vasopressor requirements, worsening abdominal distention, and increased gastric residual volume, along with an episode of emesis. The hospital nutritional-support service is consulted for feeding recommendations.
A discussion with the patient's family reveals that during the previous 6 months, she lost approximately 15% of her usual body weight and decreased her food intake because of abdominal pain associated with eating. Her preoperative body weight was 51 kg (112 lb), or 90% of her ideal body weight. The physical examination reveals mild wasting of skeletal muscle and fat. Blood tests show hypomagnesemia, hypophosphatemia, and normal hepatic and renal function. Central venous parenteral nutrition is recommended.
The Clinical Problem Malnutrition, including the depletion of essential micronutrients and erosion of lean body mass, is very common in patients who are critically ill, with 20 to 40% of such patients showing evidence of protein-energy malnutrition. The incidence of malnutrition worsens over time in patients who require prolonged hospitalization.
Protein-energy malnutrition before and during hospitalization is associated with increased morbidity and mortality in hospitalized patients. Adequate nutrient intake is critical for optimal cell and organ function and wound repair. Protein-energy malnutrition is associated with skeletal-muscle weakness, an increased rate of hospital-acquired infection, impaired wound healing, and prolonged convalescence in patients who are admitted to an intensive care unit (ICU).
However, the relationship between malnutrition and adverse clinical outcomes is complex, because malnutrition may contribute to complications that worsen nutritional status, and patients who are more difficult to feed are more critically ill and at higher risk for death and complications. Thus, the true cost of malnutrition cannot be estimated with accuracy in critically ill patients.
Pathophysiology and Effect of Therapy The pathophysiology of malnutrition in patients in the ICU is multifactorial. Critical illness is associated with catabolic hormonal and cytokine responses. These include increased blood levels of counterregulatory hormones (e.g., cortisol, catecholamines, and glucagon), increased blood and tissue levels of proinflammatory cytokines (e.g., interleukin-1, interleukin-6, interleukin-8, and tumor necrosis factor ), and peripheral-tissue resistance to endogenous anabolic hormones (e.g., insulin and insulin-like growth factor 1).
This hormonal milieu increases glycogenolysis and gluconeogenesis, causes a net breakdown of skeletal muscle, and enhances lipolysis, which together provide endogenous glucose, amino acids, and free fatty acids that are required for cellular and organ function and wound healing. Unfortunately, although plasma substrate levels may be increased, their availability for use by peripheral tissues may be blunted (because of factors such as insulin resistance and inhibition of lipoprotein lipase), and plasma levels of certain substrates (e.g., glutamine) may be insufficient to meet metabolic demands.
Critically ill patients often have a history of decreased spontaneous food intake before ICU admission, because of anorexia, gastrointestinal symptoms, depression, anxiety, and other medical and surgical factors. In addition, their food intake may have been restricted for diagnostic or therapeutic procedures. Such patients commonly have episodes of abnormal nutrient loss from diarrhea, vomiting, polyuria, wounds, drainage tubes, renal-replacement therapy, and other causes.
Bed rest, decreased physical activity, and neuromuscular blockade during mechanical ventilation cause skeletal-muscle wasting and inhibit protein anabolic responses. Drugs that are frequently administered to patients in the ICU may themselves increase skeletal-muscle breakdown (corticosteroids), decrease splanchnic blood flow (pressor agents), or increase urinary loss of electrolytes, minerals, and water-soluble vitamins (diuretics). Infection, operative trauma, and other stresses may increase energy expenditure and protein and micronutrient needs.
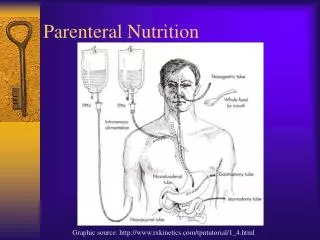
Most critically ill patients who require specialized nutrition (85 to 90%) can be fed enterally through gastric or intestinal tubes and then transitioned to an oral diet with supplements. However, in approximately 10 to 15% of such patients, enteral nutrition is contraindicated. Complete intravenous parenteral nutrition provides fluid, dextrose, amino acids, lipid emulsion, electrolytes, vitamins, and minerals.
Insulin and selected drugs may also be added. Therapeutic effects of parenteral nutrition accrue through the combined provision of energy (primarily as the dextrose and lipid components), essential and nonessential amino acids, essential fatty acids, vitamins, minerals, and electrolytes. These elements support vital cellular and organ functions, immunity, tissue repair, protein synthesis, and capacity of skeletal, cardiac, and respiratory muscles.
Nutrition Care and Assessment Chapter 17 © 2006 Thomson-Wadsworth
Nutrition in Health Care • Many medical conditions can lead to malnutrition • Poor nutrition can influence • The course of disease • The body’s response to treatment • Malnutrition – reported in 40-60% of patients hospitalized with acute illness • Healthy patients often exhibit decline in nutrition status within 3 weeks of admission © 2006 Thomson-Wadsworth
Nutrition in Health Care • Early recognition and treatment of nutritional problems • Improve effectiveness of medical treatment • Prevent complications • Registered dietician or similarly trained nutrition professional provides services to • Assess • Diagnose • Treat © 2006 Thomson-Wadsworth
Illness and Nutrition Status • Reduced food intake • Impaired digestion and absorption • Altered nutrient metabolism/excretion © 2006 Thomson-Wadsworth
Ways in Which Illness Can Affect Nutrition Status © 2006 Thomson-Wadsworth
Health Professionals and Nutrition Care • Nutrition care is often incorporated into the medical plan using: • “Critical Pathways” • “Clinical Pathways” © 2006 Thomson-Wadsworth
Health Professionals and Nutrition Care • Physicians • Prescribe diet orders (nutrition assessment and diet counseling) • Registered Dietitians • Conduct dietary assessments • Diagnose nutritional problems • Develop, implement and evaluate nutrition care plans • Plan and approve menus © 2006 Thomson-Wadsworth
Health Professionals and Nutrition Care • Nurses • Screen patients for nutrition problems – may participate in nutrition and dietary assessments • Provide diet / nutrition care • Encouraging patients to eat • Finding practical solutions to food-related problems • Recording patient’s food intake • Answering questions about specific diets • Administering tube and intravenous feedings © 2006 Thomson-Wadsworth
Health Professionals and Nutrition Care • Registered Dietetic Technicians • Work with dietician • Assist in implementation and monitoring of nutrition services • Screen patients for nutritional problems • Provide patient education and counseling • Develop menus and recipes • Ensure appropriate meal delivery • Monitor patients’ food choices and intakes • Often have supervisory positions in foodservice operations © 2006 Thomson-Wadsworth
Health Professionals and Nutrition Care • Other Health Care Professionals – Pharmacists, physical therapists, occupational therapists, speech therapists, social workers, nursing assistants, home health care aides • Assist with nutrition care • Can be instrumental in alerting dietitians or nurses to nutrition problems • May share relevant information about a patient’s health status or personal needs © 2006 Thomson-Wadsworth
Quality of Care Joint Commission on Accreditation of healthcare Organizations (JCAHO) – independent, non-profit organization that has developed an accreditation process that helps to ensure high-quality health care and awards accreditation to health care organizations based on how well standards are met. Conducts extensive on-site reviews at least once every three years. (www.jcaho.org) © 2006 Thomson-Wadsworth
Nutrition Screening • Conducted within 24 hours admission to hospital or other type of extended-care facility (JACHO) • Accurate to identify nutritional risk, yet simple enough to be completed in 5 – 15 minutes. • Conducted by nurse, nursing assistant, registered dietician or dietetic technician-- varies among health care settings. © 2006 Thomson-Wadsworth
Nutrition Screening • Often included in outpatient services and community health programs • Nutrition Screening Initiative – project sponsored by more than 25 national health, aging, and medical organizations to promote nutrition screening in the elderly © 2006 Thomson-Wadsworth
Nutrition Screening • DETERMINE – mnemonic for remembering the common warning signs of malnutrition. © 2006 Thomson-Wadsworth
Nutrition Screening • Disease. • Eating poorly. • Toothloss or mouth pain. • Economichardship. • Reducedsocial contact. • Multiplemedications. • Involuntary weight loss or gain. • Need for assistance in self care. • Elderyears (above age 80). © 2006 Thomson-Wadsworth
The Nutrition Care Process • Nutrition Assessment • Nutrition Diagnosis • Nutrition intervention • Nutrition monitoring and evaluation © 2006 Thomson-Wadsworth
Nutrition Assessment • Medical, social, and dietary histories. • Anthropometric data. • Biochemical analyses. • Physical examinations. Will be addressed in further depth in slide presentation. © 2006 Thomson-Wadsworth
Nutrition Diagnosis • Similar to nursing diagnoses • Stated in format that includes: • A specific nutrition problem • The etiology or cause • The signs and symptoms that provide evidence of the problem © 2006 Thomson-Wadsworth
Nutrition Intervention • Treatments that can improve risk factors and correct nutrition problems – including: • Dietary modifications • Nutrition handouts • Change in medication • Evidenced-based on scientific rationale and supported by results of high-quality research © 2006 Thomson-Wadsworth
Nutrition Intervention • Goals of nutrition interventions are stated in terms of: • Measurable outcomes – results of lab tests or anthropometric data • Positive changes in dietary behaviors and lifestyle © 2006 Thomson-Wadsworth
Nutrition Monitoring and Evaluation • Original goals and outcome measures are • Reviewed at previously designated dates • Compared with earlier assessment data and diagnoses • If the goals are not met • The care plan must be redesigned • Include motivation techniques or additional patient education © 2006 Thomson-Wadsworth
Historical Information • Medical History • Current complaints • Past medical conditions • Family history of illness • Surgical history • Medication history • Use of dietary/herbal supplements © 2006 Thomson-Wadsworth
Historical Information • Social History • Socioeconomic status • Cultural/ethnic identity • Educational level • Living situation • Shopping arrangements • Cooking facilities © 2006 Thomson-Wadsworth
Historical Information © 2006 Thomson-Wadsworth
Historical Information • Diet History • Dietary pattern • Dietary restrictions • Use of alcohol • Rood allergies and intolerances • Chewing and swallowing ability • Need for feeding assistance © 2006 Thomson-Wadsworth
Dietary Assessment Methods • The 24-hour recall • Food frequency questionnaire • Food record • Direct observation © 2006 Thomson-Wadsworth
Sample section of a food frequency questionnaire © 2006 Thomson-Wadsworth
Anthropometric Measurements • Height/length and weight • Height/length and weight can help assess growth in children and undernutrition and overnutrition in adults. © 2006 Thomson-Wadsworth
Anthropometric Measurements • Length • Measured in infants and children up to age two or three • Height • Measured in older children and adults See Box 17-1, p. 591. © 2006 Thomson-Wadsworth
Anthropometric Measurements • Weight • Body Mass Index (BMI) • Ideal Body Weight (%IBW) • Usual Body Weight (%UBW) • Obtaining a valid weight • Same calibrated scales • Same time of day • Same amount of clothing • After patient has voided © 2006 Thomson-Wadsworth
Anthropometric Measurements See Figure 17-4, Weight Measurement of an Infant, p. 592. See Figure 17-5, Weight Measurement of an Older Child or Adult, p. 592. See Table 17-6, Quick Estimate of Desirable Body Weight, p. 592. See Table 17-7, Use of Body Weight for Assessing Nutritional Risk, p.593. © 2006 Thomson-Wadsworth