Download
1 / 15
170 likes | 699 Views
Chlamydia in the Newborn. Sonya Mary Palathumpat, MD October 04, 2013. Introduction. Chlamydia trachomatis Most common cause of sexually transmitted infections in the United States. Chlamydia trachomatis. Gram Negative Bacterium Coccoid or Rod-shaped Obligate Intracellular Human Pathogen.

E N D
Chlamydia in the Newborn Sonya Mary Palathumpat, MD October 04, 2013
Introduction • Chlamydia trachomatis • Most common cause of sexually transmitted infections in the United States
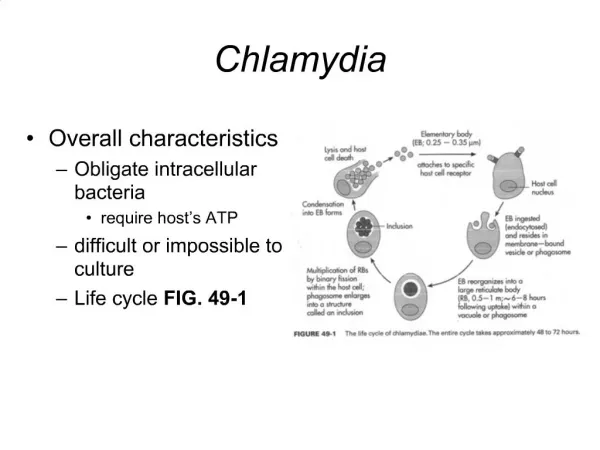
Chlamydia trachomatis • Gram Negative Bacterium • Coccoid or Rod-shaped • Obligate Intracellular Human Pathogen
Transmission • Primary mode of transmission: • Via exposure to an infected mother’s genital flora during vaginal birth • Risk of acquiring C. trachomatis in infant born vaginally to a woman with chlamydia cervicitis ~ 50 percent • Secondary mode of transmission: • After cesarean delivery with rupture of membranes
Clinical Manifestations: Chlamydia Conjunctivitis • Aka Inclusion Conjunctivitis • Most common manifestation • Likely to appear 5-14 days after delivery • Initially presents as watery discharge that becomes purulent • Can progress to swelling of eyelids with red and thickened conjunctiva (chemosis)
Clinical Manifestations: Chlamydia Conjunctivitis • Mucopurulent discharge • Pseudomembrane may form as exudate adheres to conjunctiva • Conjunctiva may become friable -> bloody discharge
Clinical Manifestations: Chlamydia Conjunctivitis • If untreated • For more than two weeks, membrane of granulation tissue may form (micropannus) • For several months, may cause corneal and conjunctival scarring
Clinical Manifestations:Pneumonia • Of infants born to mothers with cervical C. trachamatis infection, 5- 30% develop pneumonia • Affects infants at 4-12 weeks of age • Characteristic features: • Staccato cough • Type of cough that errupts in short, sudden bursts • Rales on auscultation • Occasional features: • Nasal congestion without significant discharge • Usually afebrile or with minimal fever
Clinical Manifestations:Pneumonia • Labs: • WBC: normal with elevated eosinophil count • ABG: mild to moderate hypoxemia • CXR: • Hyperinflation with bilateral, symmetrical, interstitial infiltrates
Diagnosis • Indications for testing: • Infant less than 1 mo. with conjunctivitis whose mother has a history of untreated C. trachomatis or no PNC • Infant with conjunctivitis born to mother with history of Neisseria gonorrhoeae
Diagnosis • Gold Standard • Isolation by Culture • Conjunctival and Nasopharyngeal Samples • Exudates are not adequate for testing. • Specimens must include conjunctival epithelial cells since C.trachomatis is an obligate intracellular organism
Diagnosis • Other methods of Diagnosis • Nucleic Acid Amplification (NAAT) • More rapid turnaround time for results vs Culture • Antigen Detection Methods • Direct Fluorescent Antibody Testing (DFA) • Enzyme Immunoassay Tests (EIA)
Treatment • Oral erythromycin • 50 mg/kg per day PO in four divided doses for 14 days • Treatment of both Chlamydial conjunctivitis or pneumonia • If infants fail initial course, should be retreated with second course for 14 days • Topical Therapy of Chlamydial Conjunctivitis • Not effective and there is a high failure rate compared to oral therapy
Prevention • Systemic screening and treatment of Chlamydial infection in pregnant women • CDC recommendation: • All pregnant women be screened for Chlamydia at first prenatal visit • Women under age 25 and those at increased risk for chlamydial infection should have a repeat testing in the third trimester • Pregnant women who test positive for C. trachomatis, should be treated with appropriate antibiotic therapy
References: • Chlamydia Trachomatis Infections in the Newborn. Pammi, M., Hammerschlag, M. UpToDate. 01/15/13. • Conjunctivits (Pink Eye) in Newborns. http://www.cdc.gov/conjunctivitis/newborns.html. 10/23/12