Download
1 / 33
420 likes | 1.16k Views
CHLAMYDIA. II MBBS. Intracellular Energy parasites Elementary body Reticulate body Inclusion bodies – HP, LCL Biotypes/ serotypes Tissue culture C. trachomatis Trachoma. Inclusion conjunctivitis Lymphogranuloma venereum Frei test Genital chlamydiasis C. psittaci Psittacosis

E N D
CHLAMYDIA II MBBS Dr Ekta, Microbiology, GMCA
Intracellular Energy parasites Elementary body Reticulate body Inclusion bodies – HP, LCL Biotypes/ serotypes Tissue culture C. trachomatis Trachoma Inclusion conjunctivitis Lymphogranuloma venereum Frei test Genital chlamydiasis C. psittaci Psittacosis Ornithosis C. pneumoniae KEY WORDS Dr Ekta, Microbiology, GMCA
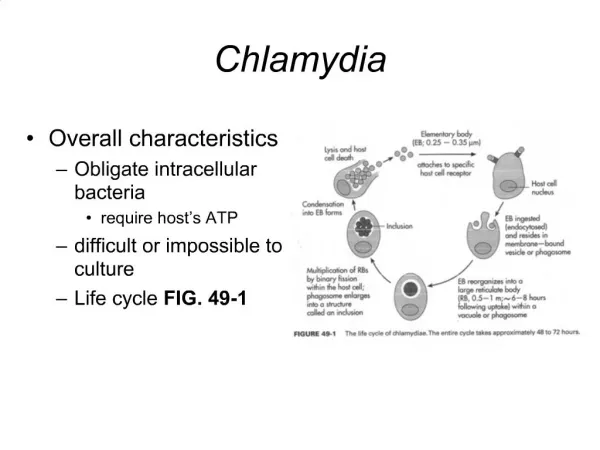
INTRODUCTION • Obligate intracellular parasites of humans, animals & birds • Resemble bacteria except it cannot multiply outside living cells/ tissues (like viruses) • Cannot synthesize ATP – depends on host cellfor energy & nutrient sources. Hence, called Energy Parasites. Dr Ekta, Microbiology, GMCA
CHLAMYDIA • 4 species in the Genus Chlamydia – C. trachomatis, C. pneumoniae, affects humans C. psittaci and C. pecorum affects ruminants • All are non-motile, gram negative; share antigens, have both DNA and RNA. Dr Ekta, Microbiology, GMCA
Classification • C.trachomatis:eye & genital infections, infant pneumonia, and LGV (Lymphogranuloma Venereum) in adults • C.pneumoniae: different types of respiratory infections. • C.psittaci : psittacosis in man, ornithosis in birds Dr Ekta, Microbiology, GMCA
Life cycle • Chlamydiae occur in 2 forms : • Elementary body – extracellular, infective form • Reticulate body – intracellular, growing & replicative form • Chlamydial microcolony within the host cell is called Inclusion body. • Mature inclusion body contains 100 - 500 elementary bodies Dr Ekta, Microbiology, GMCA
Life cycle • C. psittaci – host cell is severely damaged, EBs are released within 48 hrs by cell lysis • C.trachomatis – mature inclusion body appears to be exocytosed in 72- 96 hrs. Dr Ekta, Microbiology, GMCA
Antigenic Properties • Three major Ags • Genus specific Ag – heat stable, common to all chlamydiae, a lipopolysaccharide resembling LPS of GNB. Present in all stages. • Species specific protein Ags – present at the envelope surface, help in classifyingchlamydia into species • Ag for Intraspecies typing – found only in some members of a species, located on major OMP (MOMP), demonstrated by micro- IF. Classifies species into serovars/ serotypes Dr Ekta, Microbiology, GMCA
Variants of Chlamydia • C. trachomatis – 2 biovars: TRIC & LGV • TRIC – Trachoma, Inclusion conjunctivitis - divided into 12 serovars • LGV – Lymphogranuloma venereum – 3 serovars Dr Ekta, Microbiology, GMCA
Human diseases Dr Ekta, Microbiology, GMCA
Laboratory Diagnosis • 4 approaches available: • Microscopic demonstration of inclusion or elementary bodies • Isolation of chlamydia • Demonstration of chlamydial Ag • Demonstration of Abs or hypersensitivity Dr Ekta, Microbiology, GMCA
Microscopy • Gram negativebut stained betterbyGiemsa,Castaneda or Machiavello stains. • Giemsa Stain: Elementary body & the Reticulate body stains blue in cytoplasm • Lugol’s iodine: rapid & simple screening method for ocular infections, stains glycogen matrix of C. trachomatis • Immunoflurescence staining: more sensitive & specific, by using monoclonal Abs. Identifies inclusion bodies as well as extracellular elementary bodies. Used for ocular, cervical or urethral specimens. Dr Ekta, Microbiology, GMCA
IF staining Dr Ekta, Microbiology, GMCA
Culture • Yolk sac of 6 - 8 days old chick embryo. • Tissue culture – McCoy, HeLa cell lines * C. psittaci carry the risk of laboratory infection. Dr Ekta, Microbiology, GMCA
Microscopic appearance • A monolayer of tissue culture cells has been exposed to cells of chlamydia trachomatis. Infected cells within the cell sheet have a cytoplasm with a granular appearance. Dr Ekta, Microbiology, GMCA
Demonstration of antigens • Micro – IF : infected ocular or genital samples are stained with fluorescent conjugated Ab • ELISA – best for screening large number of specimens, detects LPS Ag • Molecular methods - PCR Dr Ekta, Microbiology, GMCA
Chlamydiatrachomatis • Leading cause of ocular & genital infections • Pathogenicities: • Trachoma • Inclusion conjunctivitis • Infant pneumonia • Genital infections – genital chlamydiasis, LGV Dr Ekta, Microbiology, GMCA
Trachoma • Greek word trakkus – rough (roughness of conjunctiva) • Caused by C. trachomatistypes A, B & C. • Chronic keratoconjunctivitis • Transmitted by fingers, fomites, flies or dust • Established trachoma passes through 4 stages (I – IV). • Infectivity is maximum in early cases, stage IV is non infectious. Dr Ekta, Microbiology, GMCA
Laboratory diagnosis of Trachoma • Demonstration of characteristicinclusion bodies(Halberstaedter Prowazek or HP bodies) in conjunctival scrapings by Giemsa. • Culture – yolk sac, cell lines Dr Ekta, Microbiology, GMCA
Treatment & Control • Local application of antibiotics • Oral administration - Tetracycline or Doxycycline for several weeks • Single dose Azithromycin • Control – mass education & chemotherapy Dr Ekta, Microbiology, GMCA
Inclusion Conjunctivitis • Caused by C. trachomatistypes D to K • Naturally present in the genital tract • Neonatal form - “Inclusion Blenorrhoea”, develops when the infant is in birth canal, appears 5-12 days after birth, prevented by local application of antibiotics • Adult form – “Swimming Pool Conjunctivitis” – associated with bathing in community swimming pools contaminated with chlamydia from genital secretions. Dr Ekta, Microbiology, GMCA
Infant Pneumonia • Usually occurs around 4-16 wks of age. • Cough & wheezing. Rarely fever • Conjunctivitis often precedes pneumonia Dr Ekta, Microbiology, GMCA
Genital Infections • Two types : • Genital chlamydiasis • Lymphogranuloma venereum Dr Ekta, Microbiology, GMCA
Genital chlamydiasis • Most common STD, clinical spectrum similar to gonococcal infections. • Men– urethritis (NGU), epididymitis, proctitis & Reiter’s syndrome • Women – acute urethral syndrome, mucopurulent cervicitis, endometritis, salpingitis, PID, infertility, ectopic pregnancy, premature delivery, postpartum fever. • Diagnosis– gram stained smears of urogenital exudates showing • more than 4 neutrophils / OIF in urethritis, • >30 / OIF in cervicitis. • Confirmatory tests – culture, micro-IF, ELISA, PCR Dr Ekta, Microbiology, GMCA
Lymphogranuloma venereum • Most commonly caused by L2 type • Site – regional lymph nodes • Incubation period – 3 days to 5 wks • 1° lesion – small painless papulovesicular lesion on external genitalia • 2° stage – after 2 wks, lymphatic spread to draining LNs (men – inguinal, women – intrapelvic & pararectal) Dr Ekta, Microbiology, GMCA
Lymphogranuloma venereum • Nodes enlarge, suppurate, become adherent to the skin & break down to form discharging sinuses. • Metastatic complications – may occur, involves joints, eyes & meninges • 3° stage – chronic, lasts for several years; scarring & lymphatic blockage • Late sequelae more distressing in women – rectal strictures, elephantiasis of vulva (esthiomene) Dr Ekta, Microbiology, GMCA
Laboratory Diagnosis of LGV • Demonstration of elementary bodies in materials aspirated from bubos (inguinal) • Isolation – cell cultures • Serology – detection of Abs • CFT 1: 64 or more • Micro- IF 1: 512 or more • Frei Test – ID test using crude chlamydial Ag, not done now. Dr Ekta, Microbiology, GMCA
Chlamydia psittaci • Causes Psittacosis– disease of parrots • Shed in the droppings or nasal discharges and aerosols are liberated. • Humans – occupational disease as in poultry workers, pigeon farmers, petshop owners, veterinarians; laboratory acquired infection • Infection by inhalation. • Mild influenza like syndrome to fatal pneumonia Dr Ekta, Microbiology, GMCA
Laboratory Diagnosis • Specimen – blood (early stages), later sputum • Demonstration of LCL (Levinthal-Cole-Lillie)Inclusion bodiesin alveolar macrophages, mouse brain, yolk sac, cell cultures • LCL bodies - more diffuse & irrregular, not stained by iodine • Serology – CFT, micro-IF Dr Ekta, Microbiology, GMCA
Chlamydia pneumoniae • Isolated in 1986 from acute respiratory diseases in adults in Taiwan – C. psittaci strain TWAR • Later classified as a separate species. • Common cause of respiratory disease in older children & adults. • C/F – pharyngitis, sinusitis, bronchitis & pneumonia (atypical pneumonia) • Outbreaks in closed communities. • Reinfections are common. Dr Ekta, Microbiology, GMCA
Chlamydia pneumoniae • Diagnosis– Ag detection by EIA, direct IF, PCR, as isolation is very difficult. • Treatment– clarithromycin or azithromycin • Newer findings – suspected to be associated withatherosclerosis and its clinical effects like coronary, carotid & cerebral arterial disease. • Evidences– detection of chlamydial Ags in plaques, isolation of chlamydia from coronary artery plaques, experimental induction of atheroma in rabbits infected with chlamydia Dr Ekta, Microbiology, GMCA
So…What’s Chlamydia anyways? How is it detected, treated and prevented? If it happens to me, what do I do? What are the possible complications? Chlamidia Dr Ekta, Microbiology, GMCA