Download
1 / 1
10 likes | 280 Views
Communication following an ectopic pregnancy: are we doing enough? An audit and service evaluation at New Cross Hospital, UK. Fatima Taki 1 Mr. J. Samra 2 1 Fourth Year Medical Student; University of Birmingham, UK 2 Consultant Gynaecologist; New Cross Hospital, Wolverhampton, UK.

E N D
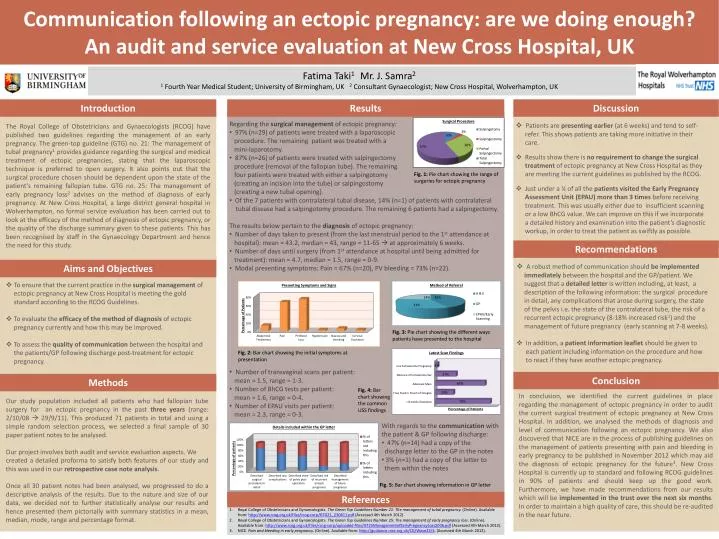
Communication following an ectopic pregnancy: are we doing enough? An audit and service evaluation at New Cross Hospital, UK Fatima Taki1 Mr. J. Samra2 1 Fourth Year Medical Student; University of Birmingham, UK 2 Consultant Gynaecologist; New Cross Hospital, Wolverhampton, UK Introduction Results Discussion • Regarding the surgical management of ectopic pregnancy: • 97% (n=29) of patients were treated with a laparoscopic • procedure. The remaining patient was treated with a • mini-laparotomy. • 87% (n=26) of patients were treated with salpingectomy • procedure (removal of the fallopian tube). The remaining • four patients were treated with either a salpingotomy • (creating an incision into the tube) or salpingostomy • (creating a new tubal opening). • Of the 7 patients with contralateral tubal disease, 14% (n=1) of patients with contralateral • tubal disease had a salpingotomy procedure. The remaining 6 patients had a salpingectomy. • The results below pertain to the diagnosis of ectopic pregnancy: • Number of days taken to present (from the last menstrual period to the 1st attendance at • hospital): mean = 43.2, median = 43, range = 11-65 at approximately 6 weeks. • Number of days until surgery (from 1st attendance at hospital until being admitted for • treatment): mean = 4.7, median = 1.5, range = 0-9. • Modal presenting symptoms: Pain = 67% (n=20), PV bleeding = 73% (n=22). • Number of transvaginal scans per patient: • mean = 1.5, range = 1-3. • Number of BhCG tests per patient: • mean = 1.6, range = 0-4. • Number of EPAU visits per patient: • mean = 2.3, range = 0-3. • Patients are presenting earlier (at 6 weeks) and tend to self- • refer. This shows patients are taking more initiative in their • care. • Results show there is no requirement to change the surgical • treatment of ectopic pregnancy at New Cross Hospital as they • are meeting the current guidelines as published by the RCOG. • Just under a ¼ of all the patients visited the Early Pregnancy • Assessment Unit (EPAU) more than 3 times before receiving • treatment. This was usually either due to insufficient scanning • or a low BhCG value. We can improve on this if we incorporate • a detailed history and examination into the patient’s diagnostic • workup, in order to treat the patient as swiftly as possible. The Royal College of Obstetricians and Gynaecologists (RCOG) have published two guidelines regarding the management of an early pregnancy. The green-top guideline (GTG) no. 21: The management of tubal pregnancy1 provides guidance regarding the surgical and medical treatment of ectopic pregnancies, stating that the laparoscopic technique is preferred to open surgery. It also points out that the surgical procedure chosen should be dependent upon the state of the patient’s remaining fallopian tube. GTG no. 25: The management of early pregnancy loss2 advises on the method of diagnosis of early pregnancy. At New Cross Hospital, a large district general hospital in Wolverhampton, no formal service evaluation has been carried out to look at the efficacy of the method of diagnosis of ectopic pregnancy, or the quality of the discharge summary given to these patients. This has been recognised by staff in the Gynaecology Department and hence the need for this study. Fig. 1: Pie chart showing the range of surgeries for ectopic pregnancy Recommendations Aims and Objectives • A robust method of communication should be implemented • immediately between the hospital and the GP/patient. We • suggest that a detailed letter is written including, at least, a • description of the following information: the surgical procedure • in detail, any complications that arose during surgery, the state • of the pelvis i.e. the state of the contralateral tube, the risk of a • recurrent ectopic pregnancy (8-18% increased risk1) and the • management of future pregnancy (early scanning at 7-8 weeks). • In addition, a patient information leaflet should be given to • each patient including information on the procedure and how • to react if they have another ectopic pregnancy. • To ensure that the current practice in the surgical management of • ectopic pregnancy at New Cross Hospital is meeting the gold • standard according to the RCOG Guidelines. • To evaluate the efficacy of the method of diagnosis of ectopic • pregnancy currently and how this may be improved. • To assess the quality of communication between the hospital and • the patients/GP following discharge post-treatment for ectopic • pregnancy. Fig. 3: Pie chart showing the different ways patients have presented to the hospital Fig. 2: Bar chart showing the initial symptoms at presentation Conclusion Methods Fig. 4: Bar chart showing the common USS findings • In conclusion, we identified the current guidelines in place regarding the management of ectopic pregnancy in order to audit the current surgical treatment of ectopic pregnancy at New Cross Hospital. In addition, we analysed the methods of diagnosis and level of communication following an ectopic pregnancy. We also discovered that NICE are in the process of publishing guidelines on the management of patients presenting with pain and bleeding in early pregnancy to be published in November 2012 which may aid the diagnosis of ectopic pregnancy for the future3. New Cross Hospital is currently up to standard and following RCOG guidelines in 90% of patients and should keep up the good work. Furthermore, we have made recommendations from our results which will be implemented in the trust over the next six months. In order to maintain a high quality of care, this should be re-audited in the near future. • Our study population included all patients who had fallopian tube surgery for an ectopic pregnancy in the past three years (range: 2/10/08 29/9/11). This produced 71 patients in total and using a simple random selection process, we selected a final sample of 30 paper patient notes to be analysed. • Our project involves both audit and service evaluation aspects. We • created a detailed proforma to satisfy both features of our study and this was used in our retrospective case note analysis. • Once all 30 patient notes had been analysed, we progressed to do a descriptive analysis of the results. Due to the nature and size of our data, we decided not to further statistically analyse our results and hence presented them pictorially with summary statistics in a mean, median, mode, range and percentage format. • With regards to the communication with the patient & GP following discharge: • 47% (n=14) had a copy of the • discharge letter to the GP in the notes • 3% (n=1) had a copy of the letter to • them within the notes Fig. 5: Bar chart showing information in GP letter • Royal College of Obstetricians and Gynaecologists. The Green Top Guidelines Number 21: The management of tubal pregnancy. (Online). Available from: http://www.rcog.org.uk/files/rcog-corp/GTG21_230611.pdf (Accessed 4th March 2012). • Royal College of Obstetricians and Gynaecologists. The Green Top Guidelines Number 25: The management of early pregnancy loss. (Online). Available from: http://www.rcog.org.uk/files/rcog-corp/uploaded-files/GT25ManagementofEarlyPregnancyLoss2006.pdf (Accessed 4th March 2012). • NICE. Pain and bleeding in early pregnancy. (Online). Available from: http://guidance.nice.org.uk/CG/Wave23/4. (Accessed 4th March 2012). References