Download

1 / 55
670 likes | 1.32k Views
Gram positive bacilli of medical importance. Vineet K. Singh, Ph.D. Department of Microbiology/Immunology ATSU/Kirksville College of Osteopathic Medicine. Aerobic spore-formers Bacillus anthracis Bacillus cereus. Regular Rods Listeria Erysipelothrix. Anaerobic spore-formers

E N D
Gram positive bacilli of medical importance Vineet K. Singh, Ph.D. Department of Microbiology/Immunology ATSU/Kirksville College of Osteopathic Medicine
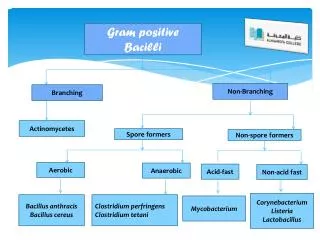
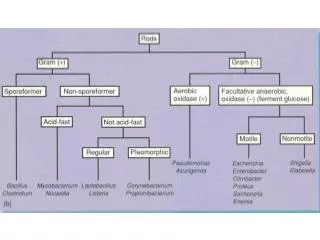
Aerobic spore-formers • Bacillus anthracis • Bacillus cereus Regular Rods • Listeria • Erysipelothrix Anaerobic spore-formers • Clostridium perfringens • Clostridium tetani • Clostridium botulinum • Clostridium difficile Irregular Rods • Corynebacterium • Propionibacterium • Mycobacterium (Acid fast) • Actinomycetes, Nocardia Gram positive bacilli
Bacillus anthracis - Key facts • "Black Bane" that swept through Europe in the 1600s was likely anthrax. • Caused significant human and animal deaths. • 1st disease to fulfill Koch's postulates (microbial etiology confirmed). • First bacterial disease for which immunization was available (1881). • Anthrax represents the single greatest biological warfare threat. • WHO estimate: release of 50kg of anthrax spores along a 2km line upwind of a city of 500,000 will lead to 125,000 (25%) infections and 95,000 deaths in 3 days.
Bacillus anthracis Characteristics: • Large (1X3-8 mm), Gram (+)ve, non-motile, spore forming (not in clinical samples) rod. • Spores resistant to heat, UV, -radiation, disinfectants; can stay dormant for decades. • Nonfastidious, non-hemolytic, medusa headcolonies, firmly adherent to agar surface.
B. anthracis – Epidemiology Primarily a disease of herbivores, especially grazing herbivores. Human infection - by contact with products of infected animals. Human to human transmission has not been documented. May be serious where animal vaccination is not practiced. Human infections - rare in the US (95% inoculation, 5% inhalation).
Genes encode protein for capsule synthesis. Unique capsule - polyglutamate, antiphagocytic capA, capB, capC pXO1 184.5 kb pXO2 95.3 kb atxA AtxA - regulates toxin & capsule production. lef – lethal factor (LF) pag – protective antigen (PA) cya- edema factor (EF) PA - responsible for cellular binding & entry. LF - a zinc protease. EF - calmodulin dependent adenylate cyclase. lef, pag, cya Toxin proteins combine to form binary exotoxins • Lethal toxin (LeTx): PA + LF Edema toxin (EdTx): PA + EF • LeTx: causes cell death; EdTx: causes massive edema, inhibits phagocytosis. 2 large plasmids (pXO1 & pXO2) account for all the virulence
Entry and actions of anthrax toxin • PA binds to anthrax receptor (ANTXR) & is processed by furin on the cell surface. • PA oligomerize into a 7 member ring and generate binding site for EF & LF. • Toxins endocytosed; acidic pH changes conformationalof PA; toxins into cytosol. • EF: an adenylate cyclase - raises cAMP; LF: protease that degrades MAPKK.
Abrasion Ingestion Inhalation Patho-physiology of anthrax
Anthrax (a Greek word) – means coal. Head, neck, & extremities - most commonly affected. Primary lesion - nondescript (painless papule, no pus). In 2-3d, form vesicles, undergo central necrosis & drying. Eshar surrounded by eroded areas & massive edema. Can be self-limiting, lesions may resolve without scarring. ~10% untreated cutaneous anthrax systemic anthrax. Characteristic black eschar Cutaneous anthrax
In <2d, an itchy skin lesion. • May later blister & rupture. • Results in a black ulcer. • Untreated - bacteremic & fatal. Early lesions on the neck Cutaneous anthrax
Inhalational anthrax (Woolsorter's Disease) • Initial symptoms: like a viral URT infection (fever, cough, myalgia, malaise). • Widened mediastinum (evidence of hemorrhagic mediastinitis), pleural effusions. • In 1-3d a fulminant course - dyspnea, strident cough, chills. Usually fatal. • Gastrointestinal & leptomeningeal lesions due to hematogenous spread. • Only 20% survived who contracted spores accidentally released from the biologic facility in Yekaterinburg(formerlySverdlovsk of Russia). All who died (66/79) were 24 y or older.
Chest radiograph showing mediastinal thickening (arrows) Inhalational anthrax
Intestinal anthrax Human intestinal mucosal edema • Occurs by eating meat from infected animal (cattle, goat, other herbivores). • Typical initial symptoms are nausea, loss of appetite, vomiting, and fever. • Subsequently - abdominal pain, vomiting (blood), severe diarrhea. 25-60% fatal.
Anthrax hemorrhagic meningitis Skin is the most common portal of entry, bacteria spreads to CNS. May also occur in cases of inhalational & gastrointestinal anthrax. ~100% fatal; extensive edema, bloody CSF with Gram (+)ve bacilli. Extensive hemorrhage of the leptomeninges (‘Cardinal’s cap appearance).
B. anthracis vegetative cells and spores Identification of Bacillus anthracis Specimens for identification Cutaneous anthrax: Vesicular stage: vesicular fluid;Eschar stage: eschar material. Gastrointestinal anthrax: Blood, stool, rectal swab. Inhalational anthrax: Blood, sputum.
Close up of colonies Tenacity of colonies Colonies of B. anthracis on SBA plates • 2-5 mm in diameter, non-motile, catalase-positive, non-hemolytic. • Flat or slightly convex colonies, irregularly round. • Comma-shaped projections from the edge (‘Medusa-head’ colony). • Contact the state public health laboratory if B. anthracis is suspected.
Identification of B.anthracis. Gram stain Vesicular fluid Ascitic fluid Blood, CSF Suspect presumptive diagnosis Smear Polychrome methylene blue Motility (non-motile) Nutrient broth Sheep blood agar Non-hemolytic gray colonies Culture Rough creamy-white colonies with ground glass appearance PLET (mixed flora) Polychrome methylene blue stain Capsules test CONFIRMATORY REPORT Lysis by g phage Susceptibility to penicillin G Polymerase chain reaction (PCR)
Bacillus cereus • Bacillus species other than B.anthracis are opportunistic pathogens. • Many have been documented to cause disease, B. cereus is most important.
B. cereus Characteristics: • Large facultativeGram (+)ve spore forming rods; non-fastidious. • b-hemolytic on sheep blood agar (helps in differentiation from B. anthracis). Epidemiology: • Cells or spores - everywhere in the environment (soil, dust, air). • Acquired from contaminated food (dairy products, rice & cooked oriental foods, meats, bakery products) or from penetrating injuries (e.g. to eye).
B. cereus Virulence factors: • Enterotoxin: • Heat-labile (diarrheal) - stimulates adenylate cyclase-cAMP, slow onset. • Heat-stable (emetic) – rapid onset. • Necrotic toxin - heat-labile enterotoxin. • Cereolysin: a hemolysin; phospholipase C: a lecithinase (eye destruction).
B. cereus infections Diarrheal syndrome Gastrointestinal infections Emetic syndrome LOCAL Wound – postoperative, burns, abscess, trauma. Ocular – conjunctivitis, panophthalmitis, endophthalmitis, keratitis. Osteomyelitis, arthritis. Non-gastrointestinal infections SYSTEMIC Septecemia, endocarditis, Respiratory, CNS
Spores & and vegetative bacteria contaminate many foods Rice, pulses Various foods Spores survive cooking germinate & multiply in food Cooking kills cells, spores survive germinate when cooled to RT Organism ingested. Heat stable enterotoxin produced in food; survive reheating (e.g., fried rice) Enterotoxin (heat labile) produced in gut Enterotoxin ingested Rapid onset vomiting Diarrhea B. cereus – food associated infections
Identification of B. cereus Food poisoning (diarrheal/emetic) Other (eye & wound swabs, blood, CSF) Vomitus or feces Food homogenate Culture on KG, MYP, PEMBA, PEMPA Mormhology: Gram stain (+)ve, spore stain (+)ve, motile Biochemistry: • Facultative anaerobe, nitrate reducer • no urease or indole production • Starch hydrolysis: emetic strains (-), other strains (+) • Acid from sugars: • Glucose, maltose, sucrose (most) - YES • Lactose, arabinose, xylose, mannitol - NO KG – Kim and Goepfert; MYP – mannitol-egg yolk-polymyxin; PEMBA & PEMPA – polymyxin-pyruvate-egg yolk-mannitol with bromothymol blue or bromocresol purple.
Characteristic B. anthracis B. cereus Growth requirement for thiamin + - Hemolysis on sheep blood agar - + Glutamyl-polypeptide capsule + - Lysis by gamma phage + - Motility - + Growth on chloral hydrate agar - + String-of-pearls test + - Differentiation of B. anthracis & B. cereus
ANAEROBIC SPORE-FORMERS • All gram (+)ve anaerobic spore formers were grouped in genus Clostridium. • Inability to reduce sulfate & cell wall are other features that defines the genus. • Currently more than 177 species in the genus, only few are pathogenic. • Ubiquitous in soil, water, sewage, normal flora of human and animal GIT. Clostridium
Clostridium perfringens Characteristics: • Large Gram (+)ve spore forming anaerobic rods. • Spores seen rarely during in vivo or in vitro growth. • More aerotolerant than other clostridia, generation times about 7 min. • Five serotypes (A-E) based on toxins. Epidemiology: • Spores/vegetative bacteria are widespread in soil & normal flora of man & animals. • Infections may be endogenous or exogenous. • Endogenous - wound contaminated by patient’s own fecal flora. • Exogenous - wound contamination by soil or by eating contaminated food.
At least 12 toxins and enzymes involved in pathogenesis FACTOR BIOLOGIC ACTIVITY a-toxin Produced by all 5, a phospholipase C, increases vascular permeability (VP). b-toxin Intestinal stasis, loss of mucosa, progresses to enteritis necroticans (pig bel). e-toxin A protoxin (activated by trypsin), increases VP i-toxin A binary toxin (an ADP ribosylase), necrotizing activity, increases VP d-toxin Hemolytic q-toxin Heat- and oxygen-labile hemolysin, cytolytic k-toxin Collagenase, gelatinase, necrotizing activity. l-toxin Protease m-toxin Hyaluronidase n-toxin DNase, hemolysin, necrotizing activity. Enterotoxin Alters membrane permeability in ileum (cytotoxin, enterotoxic), SAg. Neuraminidase Alters cell surface ganglioside receptors; promotes capillary thrombosis. Virulence factors
a-toxin Causes lysis of host cell membrane & extensive necrosis causes abscess formation, anemia, leukopenia via cell lysis
C. perfringens diseases Soft tissue infections Gastroenteritis Cellulitis Suppurative myositis Myonecrosis Food poisoning Necrotizing enteritis
Enters tissues following surgery/traumatic injury. Damage to arteries in tissues reduces oxygen supply. Clostrdia multiply & anaerobic cellulitis develops (~5d). Dosn’t involve the muscle, <aggressive than gas gangrene. Patient suffered a compound fracture of the tibia Suppurative myositis Suppuration in the muscle planes without necrosis or systemic symptoms. Clostridial cellulitis
Myonecrosis (Gas gangrene) An aggressive, highly lethal infection, toxins cause progressive muscle injury. Intense pain within a week after clostridia enters tissues due to trauma or surgery. Rapid and extensive muscle necrosis, shock, renal failure, death within 2 days. Gas in tissues due to replicating organism (hence the name – gas gangrene). Extensive hemolysis, bacteria-present; inflammatory cells-absent (due to lysis). Myonecrosis – requires aggressive surgical debridement (sometimes amputation).
Food poisoning: • Common but underappreciated; short incubation (8-22h) - continues for 12-48h. • Enterotoxin (A&C) probably responsible. • Abdominal cramps, watery diarrhea (no fever, nausea, or vomiting). Necrotizing enteritis (enteritis necroticans or pig-bel): • Acute necrotic destruction of jejunum, ulceration of small intestine (b-toxin-major role). • Peritonitis, abdominal pain, vomiting, bloody diarrhea, shock; 50% fatal. Septicemia: • Myonecrosis & necrotizing enteritis patients are bacteremic - massive hemolysis. • Caution: Correlate the presence of clostridia in blood with other clinical findings. • Significant infections are typically associated with massive hemolysis.
C. perfringens food associated infection Rare Common Enterotoxin producing type ‘A’ strains b-toxin-producing ‘C’ strains Organisms and spores in animal guts and soils Contaminated raw meat products Inadequately cooked meat, especially pork Spores survive cooking, germinate and multiply Large number ingested by person with low protein diet (inadequate intestinal trypsin) Organisms survive mild-reheating, large number ingested Enterotoxin produced in large intestine Organisms produce b toxin in small intestine damage of intestinal epithelium, protein loss into lumen Acute necrotizing disease (“Pig-bel”) Abdominal pain, bloody diarrhea 50% fatal from intestinal perforation Diarrhea
Identification of C. perfringens. • A non-motile, Gram (+)ve rod; nitrate reducer, produces acid and gas from lactose. • Presence of rods with no leukocytes in a clinical sample is a good indicator. • Black colonies on tryptose-sulfite-cycloserine (TSC) agar; liquefies gelatin within 48 h. • Nagler reaction: a-toxin gives an opaque region around growth on an egg yolk plate. Nagler reaction
Spores show round terminals (drumstick). Clostridium tetani
Characteristics: • Large (0.5X2.1-18 mm), motile, spore forming, Gram (+)ve rod, strict anaerobe. Epidemiology: • Common in fertile soil, transiently colonizes animal and human GIT. • ~1m tetanus worldwide, ~40 in the US (in elderly with waning immunity). • Most cases in developing countries are in newborns.
Virulence factors - C. tetani produces 2 potent toxins 1. Chromosomally encoded oxygen labile hemolysin - tetanolysin: • Role in pathogenesis is not clear. • Similar to SLO and hemolysin produced by C. perfringens. 2. Plasmid encoded oxygen labile neurotoxin - tetanospasmin (tetanus toxin): • Stationary phase toxin, blocks release of inhibitory neurotransmitters. • Responsible for clinical manifestations of tetanus. • Acts at myoneural and neural-neural junctions to cause muscle spasms.
C. tetani diseases • Incubation period depends on distance between site of primary infection & CNS. • Generalized tetanus: • Most common form that involves masseter muscles (trismus, lockjaw). • Sardonic smile due to contraction of the facial muscle (risus sardonicans). • Other early signs: drooling, irritability, persistent back spasms (opisthotonus). Localized tetanus: Confined to the musculature of the primary site of infection. Cephalic tetanus: If head is the primary site of infection, poor prognosis.
Trismus Risus Sardonicans Opisthotonus C. tetani diseases
Common in developing countries (mothers lack immunity). Usually acquired through contamination of the umbilical stump. Unclean tools to sever cord, cloths, soil, dung, to the stump. Excessive crying, trismus, tetanic spasms, and opisthotonus. > 90% fatal, developmental defects in survivors. Neonatal tetanus (tetanus neonatorum)
Identification • Gram positive strict anaerobe; metronidazole sensitive (all Clostridia). • Colonies on blood agar: Fine spreading growth, may appear b-haemolytic. • Very little biochemical activity useful for identification. • Round, terminal spores with “tennis racquet” appearance. • Presence of toxin (Mouse injection and survival ± antitoxin).
C. botulinum Characteristics: • A heterogeneous group of large (0.6-1.4 X 3.0-20 mm) Gram (+)ve rods. • Fastidious, strict anaerobe, species divided into 4 groups. Epidemiology:Ubiquitous, spores found in soil worldwide, disease uncommon in the US. Group Neurotoxin Phenotype I A, B, F Proteolytic, saccharolytic II B, E, F non-proteolytic, saccharolytic III C, D Weakly-proteolytic, saccharolytic IV G Weakly-proteolytic, asaccharolytic
Virulence factors • 7 neurotoxin (A-G) - 7 serotypes (each produce 1 toxin); A,B,E & F cause most diseases. • Toxins are heterodimeric proteins usually complexed with non-toxic proteins. • Toxins inactivate protein that regulates Ach release at peripheral cholinergic receptors. • Flaccid paralysis due to neurotransmission inhibition; recovery requires regeneration.
Diseases: 4 forms of botulism Foodborne botulism: • <30/yr in the US; by ingestion of preformed toxin in food. • Initial symptoms: blurred vision, constipation, abdominal pain, no fever. • 10% mortality (70% in the past), death due to respiratory paralysis. Infant botulism: • ~100/yr in the US; by toxin formed in gastrointestinal tract. • Affects infants (<1y), organism can’t survive in adults GIT. • Symptoms: initially non-specific (constipation, weak-cry). • Flaccid paralysis, respiratory arrest possible (only 1% fatal). Wound botulism: By toxin produced by the organism in wound, very rare. Inhalational botulism: Bioterrorism concern; toxin can be aerosolized (rapid onset).
Hemifacial spasm and botulinum toxin A patient before and after being treated with botulinum-A anti-toxin. Improves hemifacial spasm in > 90% of patients. Infant botulism
Identification of Clostridium botulinum On blood agar under strict anaerobic conditions – iridescent colonies due to lipase. Presence of toxin (mouse injection and survival ± antitoxin). Hydrolyzes gelatin, ferments glucose;