Download
1 / 40
420 likes | 692 Views
Progesterone…We can prevent some prematurity if we try. James Keller MD. OBJECTIVES. To review early studies concerning progesterone use in the management of preterm labor To review recent studies concerning progesterone use to prevent preterm delivery

E N D
Progesterone…We can prevent some prematurity if we try James Keller MD
OBJECTIVES • To review early studies concerning progesterone use in the management of preterm labor • To review recent studies concerning progesterone use to prevent preterm delivery • To review safety issues surrounding progesterone use in pregnancy
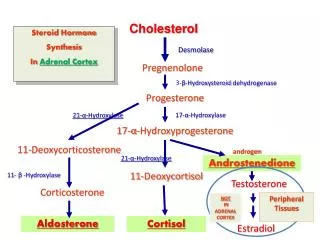
MECHANISM OF ACTION OF PROGESTERONE • Inhibit formation of myosin light chain kinase • Inhibit release of calcium • Inhibition of the formation of gap junctions • Blocking of the action of oxytocin • May inhibit production of or block action of prostaglandins • All of the above keep uterine muscle from contacting in an organized regular manner-the hallmark of effective labor • In reality these considerations remain unproven in the human population
PROGESTERONE TO PREVENT PRETERM DELIVERY HISTORY AND LITERATURE REVIEW
PROGESTOGEN ADMINISTRATION IN PREGNANCY MAY PREVENT PRETERM DELIVERY BJOG 1990 Marc J N C Kierse
PROGESTOGEN ADMINISTRATION IN PREGNANCY MAY PREVENT PRETERM DELIVERY • Meta –analyses published in response to two other meta-analyses, both of which used several different progestational agents • Analysis examined only 17 alpha-hydroxyprogesterone caproate (17P) • Provides no support for use of 17P to prevent miscarriage
PROGESTOGEN ADMINISTRATION IN PREGNANCY MAY PREVENT PRETERM DELIVERY • Five of the seven trials reviewed included data on preterm delivery • All but one showed fewer preterm deliveries in the treated groups • Only two trials looked at preterm labor, which was also decreased in the treated group
PROGESTOGEN ADMINISTRATION IN PREGNANCY MAY PREVENT PRETERM DELIVERY Miscarriage X Preterm birth X Perinatal death X Odds Ratio 1.0 2.0 5.0 0.2 0.5
Prevention of Recurrent Preterm Delivery by 17 alpha-Hydroxyprogesterone Caproate
Prevention of Recurrent Preterm Delivery by 17 alpha-Hydroxyprogesterone Caproate • Patients between 15 and 20 weeks gestation recruited at 19 centers, with a previous spontaneous preterm delivery(or pprom) between 20 and 37 weeks gestation • Excluded for multiple gestation, fetal anomaly, progesterone or heparin therapy, cerclage, hypertension, seizure disorder
463 of 1039 eligible women randomized after consent, all received one placebo injection. Prevention of Recurrent Preterm Delivery by 17 alpha-Hydroxyprogesterone Caproate
Prevention of Recurrent Preterm Delivery by 17 alpha-Hydroxyprogesterone Caproate • 91.5% compliance • Local injection reactions such as soreness(34%), swelling (14%), itching(11%) and bruising(7%), were common • Local reactions more common in the 17P group
Prevention of Recurrent Preterm Delivery by 17 alpha-Hydroxyprogesterone CaproateRESULTS
Prevention of Recurrent Preterm Delivery by 17 alpha-Hydroxyprogesterone Caproate • Rate of PTD in placebo group was very high (54.9), highlighting nature of participants • 36% of treated patients still delivered preterm • 6 women and 12 women would need to be treated to prevent ptd at <37 and <32 weeks respectively
Prophylactic Administration of Progesterone by Vaginal Suppository to Reduce the Incidence of Spontaneous Preterm Birth in Women at Increased Risk: A Randomized Placebo-Controlled Double Blind Study da fonseca et al, Sao Paulo, Brazil; AJOG 2003
da fonseca et al, Sao Paulo, Brazil; AJOG 2003 • Authors state first study to use natural progestational agents • Study population included patients with singleton gestation, previous PTD, cerclage, or uterine malformation • 142 patients assigned to progesterone suppository 100 mg nightly per vagina, or placebo • Medication administered 24-34 weeks gestation
da fonseca et al, Sao Paulo, Brazil; AJOG 2003 • Many criticisms including poorly defined exclusion population, underpowered study and exclusion of 10 PPROM patients • Reanalysis with the PPROM Patients supported findings, but small sample size still leads to question • small size will be less troublesome if other studies using this protocol confirm results
PROGESTERONE AND THE RISK OFPRETERM BIRTH AMONG WOMEN WITH A SHORT CERVIXFonseca-Fetal Medicine FoundationNEJM 2007 • Only 10% of PTD occur in patients with previous PTD • 2003-2006, eight hospitals in UK, Chile, Greece • All patients having 2nd trimester sono (20-25 weeks) were offered TVU cervical length • Exclusion criteria: anomalies, ctx, srom, cerclage • Treatment arm 200 mg progesterone capsules-inserted nightly from 24-34 weeks • Primary outcome-delivery before 34 weeks
PROGESTERONE AND THE RISK OFPRETERM BIRTH AMONG WOMEN WITH A SHORT CERVIX Median 22 weeks Cx length 34 mm (0-6.7) 431 twins
PROGESTERONE AND THE RISK OFPRETERM BIRTH AMONG WOMEN WITH A SHORT CERVIX
PROGESTERONE AND THE RISK OFPRETERM BIRTH AMONG WOMEN WITH A SHORT CERVIX
PROGESTERONE AND THE RISK OFPRETERM BIRTH AMONG WOMEN WITH A SHORT CERVIXFonseca-Fetal Medicine FoundationNEJM 2007 • The study supports the use of Progesterone therapy in patients identified with a short cervix at 20 -24 weeks • Questions • Mass screenings • Length threshold
A TRIAL OF 17 ALPHAA-HYDROXYPROGESTERONE CAPROATE TO PREVENT PREMATURITY IN TWINSNICHHD NEJM 2007 • 14 sites, 2004-2006 • 16-20.5 weeks • Exclusion: monochorionic, discordant, cerclage, uterine anomaly, medical complication, heparin therapy (relative), major chronic disease, mfrt pts
A TRIAL OF 17 ALPHA-HYDROXYPROGESTERONE CAPROATE TO PREVENT PREMATURITY IN TWINS
A TRIAL OF 17 ALPHAHYDROXYPROGESTERONE CAPROATE TO PREVENT PREMATURITY IN TWINSNICHHD NEJM 2007 • Study does not support the use of 17P in twins • Triplets with same results • Did not look at present or past obstetric history-all of which has predicted response to progesterone • Dosage used same as singletons
PROGESTERONE FOR MAINTENANCE TOCOLYTIC THERAPY AFTER TREATENED PRETERM LABOUR: A RANDOMISED CONTROLLED TRIALBorna et al, Aust NZ J Obstet Gyneacol, 2008 • Seventy woman randomised to progesterone or no treatment after acute tocolysis • Progesterone given as suppositories, 400 mg daily • Woman similar with respect to history of preterm births (12%-13%) • GA at admission 31-32 weeks
PROGESTERONE FOR MAINTENANCE TOCOLYTIC THERAPY AFTER TREATENED PRETERM LABOUR: A RANDOMISED CONTROLLED TRIALBorna et al, Aust NZ J Obstet Gyneacol, 2008
Cervical length changes during preterm cervical ripening: effects of 17-α-hydroxyprogesterone caproateFachchinetti et al AJOG 2007 • Sixty patients admitted for treatment of PTL from 25-34 weeks • Patients received Atosiban and steroids for 48 hours • Patients randomized to 341 mg 17P twice weekly or observation • Patients all less than 2 cm dilated • Looked at cx length change and rate of preterm delivery
Cervical length changes during preterm cervical ripening: effects of 17-α-hydroxyprogesterone caproateFachchinetti et al AJOG 2007 CLINICAL CHARACTERISITICS
Cervical length changes during preterm cervical ripening: effects of 17-α-hydroxyprogesterone caproateFachchinetti et al AJOG 2007 RESULTS
SAFETY • Progesterone is a category D drug • Positive evidence of human fetal risk exists, but benefits in certain situations may make use of the drug acceptable despite its risks • Black Box Warning • Is this warranted?
SAFETY • All progesterones are not equal • You could not pay me enough to re-learn the differences-the key is that hydroxyprogesterone is a metabolic product of progesterone, which is produced in the corpus luteum-all pregnancies are exposed to high levels of this hormone • Progestins-may include all hormones with progesterone like activity-including testosterone derived progestins • Multiple studies have shown 17P has no androgenic activities
SAFETY • Studies suffer from confounding variables such as pregnancy complications, past history and co-administration of other drugs • The largest study to date followed 649 offspring exposed to 17P, and found only a non-significant increase in abnormal testes (1.8% vs1.2%) primarily undescended testes • The conclusion of this study, and the preponderance of reviews support the belief that there is no association between progesterone and birth defects
USE OF PROGESTERONE TO REDUCE PRETERM BIRTHACOG COMMITTEE OPINIONOCTOBER 2008 • Progesterone supplementation for the prevention of recurrent preterm birth should be offered to women with a singleton pregnancy and a prior spontaneous preterm birth due to spontaneous preterm labor or premature rupture of membranes. Current evidence does not support the routine use of progesterone in women with multiple gestations. Progesterone supplementation for asymptomatic women with an incidentally identified very short cervical length (less than 15 mm) may be considered; however, routine cervical length screening is not recommended.
SUMMARY • In a world where nothing seems to work, Progesterone seems effective in preventing PTD in subsets of high risk patients • This effectiveness, is supported by decades of studies and clinical experience