Download
1 / 1
10 likes | 138 Views

E N D
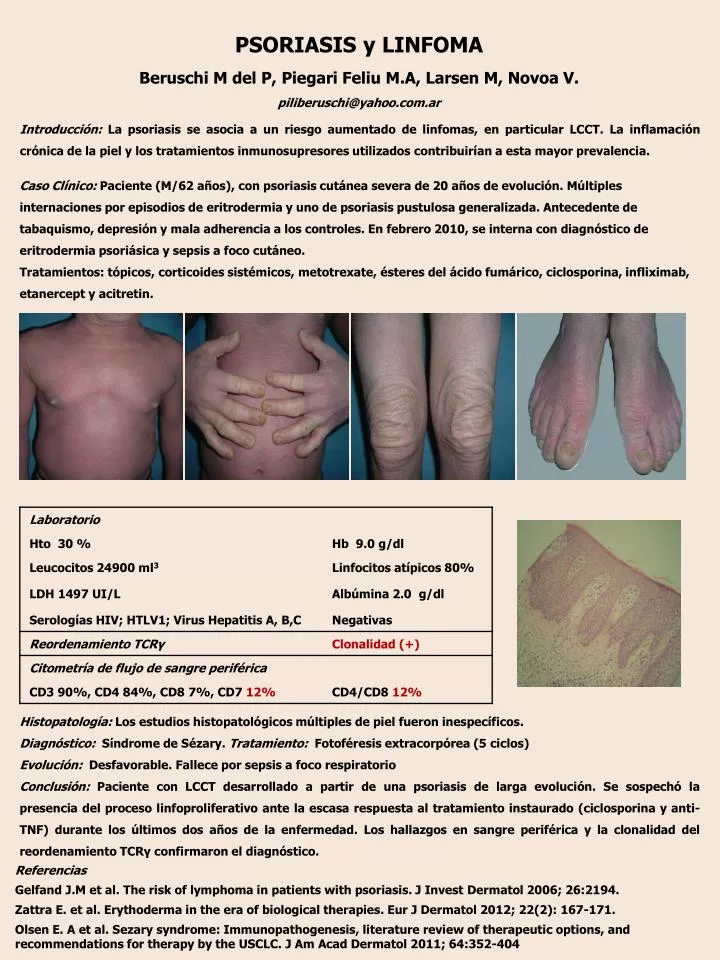
Caso Clínico: Paciente (M/62 años), con psoriasis cutánea severa de 20 años de evolución. Múltiples internaciones por episodios de eritrodermia y uno de psoriasis pustulosa generalizada. Antecedente de tabaquismo, depresión y mala adherencia a los controles. En febrero 2010, se interna con diagnóstico de eritrodermiapsoriásica y sepsis a foco cutáneo. Tratamientos: tópicos, corticoides sistémicos, metotrexate, ésteres del ácido fumárico, ciclosporina, infliximab, etanercept y acitretin. PSORIASIS y LINFOMABeruschi M del P, PiegariFeliu M.A, Larsen M, Novoa V.piliberuschi@yahoo.com.ar Introducción: La psoriasis se asocia a un riesgo aumentado de linfomas, en particular LCCT. La inflamación crónica de la piel y los tratamientos inmunosupresores utilizados contribuirían a esta mayor prevalencia. Histopatología: Los estudios histopatológicos múltiples de piel fueron inespecíficos. Diagnóstico: Síndrome de Sézary. Tratamiento:Fotoféresis extracorpórea (5 ciclos) Evolución: Desfavorable. Fallece por sepsis a foco respiratorio Conclusión: Paciente con LCCT desarrollado a partir de una psoriasis de larga evolución. Se sospechó la presencia del proceso linfoproliferativo ante la escasa respuesta al tratamiento instaurado (ciclosporina y anti-TNF) durante los últimos dos años de la enfermedad. Los hallazgos en sangre periférica y la clonalidad del reordenamiento TCRү confirmaron el diagnóstico. Referencias Gelfand J.M et al. Therisk of lymphoma in patientswith psoriasis. J InvestDermatol 2006; 26:2194. Zattra E. et al. Erythoderma in the era of biologicaltherapies. Eur J Dermatol 2012; 22(2): 167-171. Olsen E. A et al. Sezarysyndrome: Immunopathogenesis, literaturereview of therapeuticoptions, and recommendationsfortherapybythe USCLC. J Am AcadDermatol 2011; 64:352-404