Download
1 / 20
210 likes | 842 Views
HIV/AIDS. Students4Student Hugh Tulloch. Learning objectives. Go through the core information on HIV & AIDS Epidemiology Pathophysiology Signs/symptoms Investigations management. Epidemiology. 33 million people infected world wide 2.5million newly infected each year 2.1 million die

E N D
HIV/AIDS Students4Student Hugh Tulloch
Learning objectives • Go through the core information on HIV & AIDS • Epidemiology • Pathophysiology • Signs/symptoms • Investigations • management
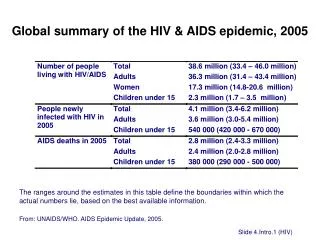
Epidemiology • 33 million people infected world wide • 2.5million newly infected each year • 2.1 million die • Around 98,400 people were living with HIV in the UK at the end of 2012, of whom 22 percent were unaware of their infection • Commonly in groups MSM and BME (black and minority ethnic) What proportion of people with HIV in UK are undiagnosed????
Pathophysiology: route of infection • Semen, cervical secretions & blood • Sexual intercourse • Genital ulceration (HSV) enhances transmission • Men women > Women men • Receptive anal partner • Mother child (vertical) • 15% without intervention • Risk factors • High viral load, advanced disease, PROM • Usually perinatally • Breastfeeding – shown to double risk of vertical transmission What are the common routes of infection??
Pathophysiology: route of infection (contd) • Reduce risk of vertical transmission • ARV • C-section • Avoid breast feeding • IVDU • Needle exchange • education
Pathophysiology: the virus • Retrovirus (uses reverse transcriptase) • HIV-1 & HIV-2 • HIV-2 is mainly just west Africa (also not as bad) • HIV-1 everywhere else • HIV divided into 3 groups (M,N,O) – M is major group • Group M is subdivided into 10 subtypes (A-J) • B is found most commonly in europe How can HIV be subdivided??
Pathophysiology: the virus What cell does HIV bind to and infect?? • HIV had surface glycoprotein (gp120) • Recognises CD4 • CD4 interacts with gp120 and CCR5 and CXCR4 (chemokine receptor) to allow HIV to enter cells • HIV RNA is incorporated into the CD4 helper lymphocytes DNA • Virons are budded off • Cell dies after 2 days • Defective T-cell homeostasis • Immuno-comprimised and tumours • HIV can also have direct effect on certain body tissues What glycoprotein on the virus membrane allows this?
Signs/symptoms: clinical pattern • Primary HIV infection • 30-80% patients experience acute syndrome around 2-4 weeks after infection • Fever, malaise and a maculopapular rash • Symptomatic HIV • Certain opportunistic diseases are regarded as AIDs defining. When these are present it suggests the development of AIDS • Eg. PCP, CMV, Toxoplasmosis, Kaposi’s sarcoma What is the rash frequently associated with a recent HIV infection??
Common opportunistic infections • Pneumocystis carinii pneumonia (PCP) • If CD4 count drops below 200 • Non productive cough, fever, dyspnoea • Treat with high dose co-trimoxazole (also can be used as prophylaxis) • Cytomegalovirus (CMV) • Very late stage disease (CD5<50) • Progessive retinitis • Regular ophthalmological screening usuful • Toxoplasmosis • Ring enhancing lesions in brain due to protozoa infection List some common opportunistic infections that are thought to be AIDS defining
Common opportunistic infections • Kaposi’s sarcoma • Caused by herpes virus • Occurs in 20% gay men with HIV • Treat with radiotherapy • HAART • Herpes zoster, oral candidiasis • Not usully considered AIDS defining but can present as CD4 count decreases
Diagnosis • Detection of anti HIV antibodies by ELISA (Enzyme liked immunosorbent assay) • Seroconversion must have occurred (latent infection, window period) • HIV RNA in plasma can be quantified – high viral loads have poorer prognosis • Anyone presenting with recurrent infections, unexplained fever or lymphadenopathy should be tested for HIV When can we test someone for HIV?
treatment • HAART • Highly active anti-retroviral therapy • Has made HIV a chronic condition • Prognosis is good if diagnosed early • 3 main classes of drug: • Nucleoside reverse transcriptase inhibitors • Protease inhibitors • Non-nucleoside reverse transcriptase inhibitors • 3 or 4 of these drugs are combined • Goal is undetectable viral load
Problems with treatment • Resistance • Side effects – neuropathy, lipodystrophy • Compliance • Other drug interactions What are some common problems with treatment?
case • A 28-year-old man had several complaints. He had a bad case of thrush (oral candidiasis) and low grade fever, had serious bouts of diarrhea, had lost 20 pounds in the last year without dieting, and, most seriously, complained of difficulty breathing. His lungs showed bilateral infiltrate on radiographic examination • 1. What laboratory tests should be done to support and confirm a diagnosis of HIV infection and AIDS? • 2. what disease caused the ‘bilateral infiltrate on radiographic examination,’ • 3. what treatment should he be started on
case • 30 year old man comes into your GP surgery with fever and malaise for 2/52. He is MSM in a long term relationship. • What tests to you offer him? • Why does resistance to HAART occur so readily in HIV? • Reverse transcriptase is error prone