Download

1 / 51
580 likes | 979 Views
Infant, Toddler, Preschool Speech/Language Intervention Related to Cleft Palate. Theresa M. Snelling, MA, CCC-SLP Pediatric Speech-Language Pathologist Clinical Coordinator Rose Cleft Palate and Craniofacial Center Denver, Colorado. REFERENCES:.

E N D
Infant, Toddler, Preschool Speech/Language Intervention Related to Cleft Palate Theresa M. Snelling, MA, CCC-SLP Pediatric Speech-Language Pathologist Clinical Coordinator Rose Cleft Palate and Craniofacial Center Denver, Colorado
REFERENCES: • Peterson-Falzone SJ, Hardin-Jones MA, Karnell MP, Trost-Cardamone JE. (2006). The Clinician’s Guide to Treating Cleft Palate Speech. St. Louis, MO, Mosby. • Kummer AW. (2008) Cleft Palate and Craniofacial Anomalies: Effects on Speech and Resonance (2nd ed.). Englewood Cliffs, NJ: Thomson Delmar Learning. • Hardin-Jones, M., Chapman, K., and Scherer, N.J. (2006, June 13th). Early Intervention in Children with Cleft Palate. The ASHA Leader. • American Cleft Palate-Craniofacial Association (2009). Parameters or the Evaluation and Treatment of Patients with Cleft Lip/Palate or Other Craniofacial Anomalies. Available from www.acpa-cpf.org.
LUKE • LUKE- Diagnosis - Unilateral Complete Cleft Lip and Palate Services – Early Intervention; Individual Private speech therapy from 3- 4 ½; Child Find Preschool 3-5 years.(NO SPEECH THERAPY CURRENTLY); GOOD PALATAL CLOSURE. Surgeries: INITIAL LIP REPAIR FOLLOWING NASO-ALVEOLAR MOLDING- 3 MONTHS; PALATE REPAIR – 11 MONTHS; 3 SETS PE TUBES.
Paige- cleft of soft palate only • Palate repair- 12 months /developed fistula; second repair –pharyngeal flap and fistula repair /developed fistula; ongoing speech therapy, pervasive HYPERNASALITY and nasal emission. Advanced language skills!! • Wore obturator • Recent re-repair 2012 = palate closure and NORMAL resonance!
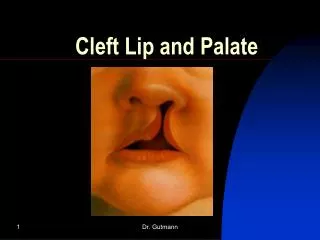
INFANT WITH CLEFT PALATE-early concerns… Feeding Speech sound development • Open palate- can’t create negative pressure for sucking • Liquid and food leak in to nasal cavity ADAPTATIONS… Feeding positioning (upright) Adapted bottle to control for lack of suck Limit feeding sessions to 20-30 minutes to limit calorie burn • Open palate can’t create oral pressure for speech sounds • Sounds needing oral pressure result in nasal airflow or nasal resonance SPEECH ADAPTATIONS… Nasal sound substitutions for oral consonants (m/b, n/d) Increased glottal sound play Nasalized vowels
Oral structures for SPEECH AND FEEDING SOFT PALATE and HARD PALATE CREATE CLOSURE BETWEEN ORAL CAVITY AND NASAL CAVITY
CHARACTERISTICS OF CLEFT PALATE SPEECH (Primary) RESONANCE DISORDERS ARTICULATION DISORDERS ***This is what I’ll cover during this first half of our presentations! (Secondary) LANGUAGE DISORDERS OR DELAY VOICE DISORDERS (Laryngeal)
RESONANCE DISORDERSWHAT DOES “NASAL” MEAN? • HYPERNASAL-excessive nasal resonance during production of VOWELS- VOWELS!!!!! • HYPONASALITY- a reduction in normal nasal resonance resulting from a partial or complete blockage of the nasal airway by any number of sources. • HYPER-HYPONASALITY (MIXED NASALITY)-the simultaneous occurrence of hypernasality and hyponasality in the same speaker usually as a result of VPI in the presence of high nasal resistance that is not sufficient to block nasal resonance completely.
NASAL EMISSION (articulation) Nasal emission- nasal air escape associated with consonants requiring high oral pressure. May or may not be audible- often seen in conjunction with hypernasality on vowels. NASAL SUBSTITUTIONS (Articulation – may overlap with hypernasal resonance and be secondary to VPI or unrepaired cleft palate!) /m/ and /n/ substitutions for consonants For example: m/p, b, w, r; n/ t, d, l, sh; ng/n, k, g
NOTE: • AVOID THE TERM- “NASAL” …”S/He sounds nasal…” does not differentiate hypo and hypernasality.
ARTICULATION • PLACE, MANNER, AND VOICING… Most errors related to cleft palate have to do with PLACEMENT errors while manner is maintained! ATTEND TO PLACEMENT!!! Usually BACKED!
Glottal stops, nasal snorts PLOSIVES /b, p, t, d, k, g/ AFFRICATES /tS, dZ/
Pharyngeal Fricatives, Nasal Fricatives Fricatives- s, z, sh, v, th, f Affricates- ch/tS/, j/dZ/
Most common articulation errors related to palatal clefts- GLOTTAL STOPS PHARYNGEAL FRICATIVES NASAL FRICATIVES NASAL PHONEME SUBSTITIONS
COMPENSATORY MISARTICULATIONS Compensatory misarticulations related to cleft palate are usually errors in PLACEMENT OF PRODUCTION. They are learned articulatory postures or placements that typically persist even after successful surgery or appliance management of the pharyngeal port and therefore co-exist with an adequate closure mechanism. They tend to be BACKED ARTICULATIONS relative to the target place of production.
VELOPHARYNGEAL INSUFFICIENCY Velopharyngeal Insufficiency (VPI) is a resonance disorder associated with a natural “pressure valve” in the back of the mouth that does not maintain air pressures that are needed in typical speech production. The disorder may be structural or functional or results in inadequate separation of the oral and nasal cavities. ***JEFF WILL COVER THIS MORE IN PART II
INSTRUMENTAL ASSESSMENT OF VPI In therapy setting • MIRROR TEST**(great with little ones!!!) • STRAW ASSESSMENT**(older children =biofeedback) In team/clinic: (JEFF will cover) • VIDEOFLOUROSCOPY • NASOENDOSCOPY/VIDEOENDOSCOPY • NASOMETRY
THERAPY TECHNIQUES…ALL AGES Goals: • TO CORRECT THE PLACEMENT ERRORS (often will improve/correct hypernasal resonance.) • Improve hypernasal resonance (if it’s structural secondary surgical management is needed- but therapy should be tried first especially in the presence of articulation errors.)
Therapy techniques…continued… • Target high pressure- oral vs. nasal. • LABEL air flow- “windy sound”, “lip popper” for direct feedback… even with little ones (15-18 months old.) • TARGET strong and varied vowels and glides /w, l, r, j, h/ if not present or weak-Children will often produce glides even in the presence of VPI.
BACKING reduction… TARGET BACKING ERRORS- move sounds anterior!!! • vowels (anterior round vowels /u/ /oe/) • glides /w, r/…not /j/ substitution • mid-dorsal IS NOT the goal… but may be the “process” of moving sounds forward (from /k/ placement, to mid-dorsal placement, to tip alveolar…) • use ‘lips’ to encourage ANTERIOR airflow- rounded lips help move air forward.
BACKING reduction… • TRY OVERPLACEMENT of articulators to decrease backing… ***/t/- produced as a /k/…I often start with tongue between lips rather than on alveolar ridge- then pull it back in mouth once they can produce plosive with tongue tip! (Sarah) Family was given /t/ to work on- Child produced “glottal stop + vowel” and in all word attempts- this was given as homework BEFORE child could produce a /t/! Approach- targeted /p/…moved to overplacement for /t/….
KEY POINTS: • Determine PLACE of articulation error and target with emphasis on manner, voicing and PLACE classifications. • Start with PLACEMENT- even pending surgery. IF YOU EMPHASIZE MANNER (plosive, fricative) with VPI- likely to teach/encourage compensatory articulation patterns.
VIDEOS E- th, t, d- GOAL “eliminate Backing”
Stella 2 ½ years Speech Therapy in the presence of Velopharyngeal Insufficiency (VPI)
IN presence of Velopharyngeal Insufficiency… IF you teach STRIDENCY for “s” or “sh” in the presence of VPI or unrepaired palate, child will create stridency in back of throat = PHARYNGEAL FRICATIVE! (TARGET ONLY ORAL, ANTERIOR AIRFLOW!!!! IF you teach “PLOSIVES” in presence of VPI- child may use GLOTTAL STOP…. Target light contact, anterior airflow, overplacement,….strategies. DON’T TEACH OR REINFORCE COMPENSATORY ARTICULATION ERRORS!!
KEY POINTS: • Rule out obvious structural issues such as a palatal fistula that does not allow for a build up of oral pressure even in the presence of a functional soft palate; may need obturator to cover fistula in the hard palate. OBTURATORS ARE POSSIBLE FROM ABOUT 3 ½ YEARS OLD (REMOVEABLE); NON-REMOVEABLE ATTACHED TO BRACKETS ON TEETH AT ABOUT 3 YEARS OLD
KEY POINTS: • Encourage strong productions-”Use Your Big Strong Mouth.” Patients frequently will try to control nasal escape related to VPI by decreasing oral strength, pressure, and volume. This does NOT contribute to optimizing VP closure. Although increasing pressure and volume may increase audible nasal emission, it may be a stepping stone allowing for contrast, and/or improved outcome even following secondary surgery (fistula repair or pharyngeal flap.)
KEY POINTS: • Use visual and tactile feedback… pop cotton, feel airstreams on your hand, see the tongue hump in the back, see air on a mirror or with SeeScape, etc… LUCY p-final
BIRTH TO 3 INTERVENTIONPlease read on own!! TEACH PARENTS/GRANDPARENTS/CARETAKERS... INDIRECT LANGUATE STIMULATION TECHNIQUES!!! • Self Talk • Parallel Talk (play by play!) • Naming/Modeling • Expansion • Motor, paired with sounds/speech CAN, AND SHOULD, PAIR WITH CLEFT PALATE GOALS AND OBJECTIVES!
PROBLEM…Child doesn’t imitate words… IMITATION DEVELOPMENT…. • Eye contact/Smile • Motor imitation (pat-a-cake, peek-a-boo, SO BIG!) • Vocal imitation (reciprocal vocalization of vowels, grunting, giggling….) • INFLECTION!! Easier to imitate- thus “UH OH!!!” “OH *#@!*” • MOTOR paired with sounds (BYE BYE, UH OH) (BABY sign!) • SOUND IMITATION – easier developmentally than words!!! TARGET SOUNDS if they are not yet imitating sound play! • WORDS, word combinations, phrases, sentences… • ESTABLISH IMITATION LEVEL…BUILD FROM STRENGTH!!!
PROBLEM…Child doesn’t imitate words… • ESTABLISH WHAT THE CHILD IMITATES…(motor movements, joint attention, feeding the baby…) • BUILD ON THAT LEVEL!! Don’t make WORDS the target when child doesn’t imitate motor actions in play- START WITH IMITATION!! • IMITATION, IMITATION, IMITATION- IN PLAY!! Child’s play, follow their lead, introduce new play schemes by playing them yourself, limit questions and commands….
PROBLEM…Child doesn’t imitate words… When Motor Imitation occurs in play- add sounds, noises, facial expressions… • Stirring food “SH, SH, SH, SH…” • Knock on doll house door “knock, knock” at same time as motor. • “SH, SH, SH… baby is sleeping” when putting doll to bed. • UH OH!! Hand to your face-EVERYTIME…when they imitate putting hands to face- it increases chance they’ll pair it with approximation of “UH OH!”
PROBLEM…Child doesn’t imitate words… WHAT ABOUT INFLECTION…? • “Whatever” • “BO BO! No!” (yelling at dog was model) • “I LOVE YOU!” (3 syllables approximated) Inflection is why kids say “uh oh”! Early! START IMITATION WHERE THEY ARE SUCCESSFUL- THAT’S THE STRATEGY!!!
SUMMARY of Indirect LanguageStimulation… • Reduce questions…especially yes/no responses. (‘choice’ questions increase the chance of a verbal response) • Don’t use commands in play- model the activity! INSTEAD: • Follow child’s lead • Model play skills • Use self talk, parallel talk, modeling, expansion. • Use exaggerated inflection (UH OH! Oh NO!) • Encourage turn-taking….2 year olds will sit in a chair and take turns- it can still be “play”.
CLEFT PALATE SPEECH APPLICATIONS… INFANTS: Make sure parents know that sounds infant pre-palate repair CAN make are “M, N, NG, vowels, gurgles” Talk and imitate child’s sound play…don’t push sounds they CAN’T make (plosives, fricatives, affricates.) ******Good sounds to target during play in EARLY INTERVENTION- vowels (increase variety), /w, r/, /l/,/m, n/.
USE INDIRECT LANGUAGE TECHNIQUES BUT… HAVE SPECIFIC SOUND AND RESONANCE GOALS! • EATING/CHEWING SOUNDS – to get lip smacks! • Stacking blocks- Put block to face- make BIG OPEN VOWEL SOUNDS…you put block on…then give block to child “your turn”…don’t tell them to say it at first…FIRST get the game of turn-taking (motor) then add sound…then modify sound…”POP IT!” “BIG MOUTH!” • Animal sounds, car sounds,… CHOOSE HIGH PRESSURE PHONEMES IF PALATE IS REPAIRED!!!!
BOOKS… CHOSE BOOKS AND TARGET WORDS TO FACILITATE HIGH PRESSURE SOUND DEVELOPMENT… “Where’s Spot?” BOOK = “NO PUPPY!” Child’s response to tell mommy dog…”NO PUPPY!” “DID YOU FEEL THE AIR POP? PUPPY!!” Pop air on their hand- let them pop it on your hand… This is a great combined language and articulation goal= 2 word combinations AND high pressure (plosive) sound production!!
STRIDENCY… • Dolls: “sh!” for sleeping- targeting fricatives! • FOOD/KITCHEN play- “HOT!” Big open air on /h/ to work towards stridency in “sh”… • SNAKES- Snake sounds!! “ssss” • “Shwoosh”- paired with other sounds. • Paper/markers- make long lines or circles to represent continuant feature of /s/, ‘sh’, /f/…pair sound with the motor.
HIGH PRESSURE PHONEMES… • Coloring paper/markers- P, B- “lip poppers”- pair sound with any motor activity. “Tap” marker on paper for /p/ or /t/… • Train set…”ch, ch, ch… Target “pop” component of the “ch” (the /t/). • /k/ = back scraper; /t tongue tapper; /p/ “popper”- and “feel” the air on your hand!!
WHAT IF PALATE IS UNREPAIRED OR CHILD HAS VPI? • Target BIG OPEN vowels!!! • Target anterior lip movement on vowels (“oh”, “oo”, “ow”…) • Target Glides- yes even /l/!! Many 2 years olds CAN make an /l/, and if they’re stimulable it will usually not result in a compensatory articulation error. • Target Glides- I work on both /w/ and /r/ when they are backed or omitted altogether in words- ROUND ANTERIOR LIPS move the glide forward through the mouth- THIS IS HOW YOU IMPROVE ORAL MOTOR LIP AND TONGUE AND CHEEK STRENGTH!! IN WORDS AND SPEECH! NOT blowing exercise!
WHAT IF PALATE IS UNREPAIRED OR CHILD HAS VPI? • DON’T teach glottal stops, pharyngeal fricatives or nasal fricatives… on accident! If palate is open or too short, but not yet ready for surgery… be very aware of your targets!! To get good lip use, target /m/ words and tread lightly with a STRONG /b/- will get a paired glottal stop! (Chu Chu)
WHAT IF PALATE IS UNREPAIRED OR CHILD HAS VPI? TARGET Glides and BIG vowels to increase intelligibility! More accuracy on vowels with improve intelligibility even in the presence of VPI! VOICELESS plosives /p,t, k/are easier to approximate if VPI is present and less likely to be paired with a glottal stop than VOICED cognate /b,d, g/. Target voiceless, with light contact
PRIOR TO PALATE REPAIR: • Target IMITATION!! Not necessarily specific sounds, but the GAME OF IMITATION! This goal lays the ground work for speech therapy post palate repair. • Target more than just receptive language skills- expanding play skills and motor imitation. • Reciprocal vocalizations- develop between 6-9 months- play with vowels and inflection and facial expressions.
AFTER palatal repair: Teach the contrast of oral vs. nasal by using terms like- • “that was in your mouth!” • “Uh Oh, that was in your nose!” (my nose too!) • Target- big, open vowels…and high pressure consonants (plosives, fricatives and affricates)… IN THE CONTEXT OF PLAY!!!
GOALS AND OBJECTIVES: HAVE specific targets…related to resonance, articulatory placement, and compensatory articulation patterns: • High pressure phonemes (even with 18 month olds). • Stridency (sh, s) in sound play or words. • Glides (w) using lip rounding. • Develop big open vowels to reduce Hypernasality. • If connected speech is mumbled with poor intelligibility- target “use your big, strong mouth”.
GOALS AND OBJECTIVES: PROGRESS reports should include information about: • Resonance. • Articulatory placement patterns. • Strategies that worked to address goals. • Compensatory articulation errors. GOAL: “…will use plosives /p, t, k/ in single words…” BE SURE to document error pattern as glottal stop, or nasal substitution or omission of consonants with vowels only sound used…
REPORTS! • INCLUDE DETAILS RELATED TO CLEFT PALATE IN YOUR REPORTS… IT’S CRITICAL TO THE DECISIONS THE CLEFT PALATE TEAM HAS TO MAKE OVER TIME! • TO DETERMINE IF SECONDARY SURGICAL MANAGEMENT IS NECESSARY- IT’S IMPORTANT TO KNOW WHAT HAS BEEN TARGETED IN THERAPY!!
HAVE GOALS! • More than just language stimulation with young children (birth to 3)… have “specific” goals for articulation and resonance development related to cleft palate. • Speech therapy is still appropriately ‘play based’ but that does not mean you avoid articulation and resonance goals… *BIG OPEN MOUTH *STRONG,VARIETY OF VOWEL *SOUNDS, PAIRED WITH MOTOR IMITATION, TO INCREASE VARIETY OF VOWELS AND CONSONANTS PRODUCED.
REMEMBER… • BLOWING AND SUCKING EXERCISES DO NOT IMPROVE CLOSURE FOR SPEECH (they might improve blowing and sucking…but the goal?????) • No clinical, scientific research to support the benefit to cleft palate speech error patterns for isolated blowing and sucking exercises! SPEECH/SOUND correlation needed for speech improvement…