Download
1 / 29
300 likes | 393 Views
Learn about the effects of high altitude on the human body, including hypoxia, acclimatization, and altitude sickness. Understand how the body adapts to low oxygen levels and the risks associated with high altitudes.

E N D
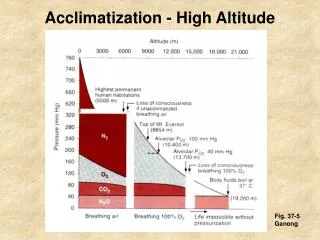
SIGNIFICANT ATMOSPHERIC PRESSURE VARIATION WITH ALTITUDE: PRESSURE ALTITUDE (FEET) ( mm of Hg) (ATMOSPHERIC UNIT) 0 760 1 18,000 380 1/2 34,000 190 1/4 48,000 95 1/8 63,000 47 1/16
BASIC CONCEPT: Human body is specifically designed in such a way that it delivers adequate O2 to the tissues only when oxygen is supplied at a pressure close to the sea-level (P = 760 mm Hg PO2 =159 mm Hg) So, at high altitude there is hypoxic hypoxia tissue oxygenation suffers physiological derangements. “connecting a 24 volt motor to a 6 volt battery”—perfect comparison by J.S.Milledge.
ALTITUDES & HEIGHTS • Normally most people on earth stay at around the Mean Sea Level (MSL) • However, groups of people stay at higher than normal attitudes. • The Sherpas, a mountain tribe of Himalayas live at around 5500 Meters above MSL, normally. • When people living around MSL go up to higher altitudes, changes occur in their physiology, especially in Respiration.
BAROMETRIC PRESSURE CHANGES IN HIGH ALTITUDE • As the altitude increases above the sea level, the corresponding atmospheric pressure decreases. • The partial pressure of Oxygen also decreases. • The arterial Oxygen saturation levels also decrease with increase in the altitude.
ACUTE EFFECTS OF HYPOXIA • As the altitude increases, the barometric pressure decreases. • This causes a handicap which may be: • Appreciable • Considerable • Serious • Causing Imminent Collapse
ACCLIMATIZATION • “Getting used to…” • People remaining at high altitudes for days, weeks or years become more and more acclimatized to low PO2. • This causes the hypoxia to cause fewer deleterious effects on their bodies. • They can thus work harder at higher altitudes without hypoxic effects.
How does acclimatization occur? • Increased : • Pulmonary ventilation. • Number of RBCs ( Hypoxia causes excess erythropoiesis). • Diffusing capacity of the lungs. • Vascularity of the peripheral tissues • Ability of the tissue cells to use Oxygen despite low PO2.
NATURAL ACCLIMATIZATION • This occurs in people living from their birth at high altitudes. • Those living in the Andes & Himalayan mountains, for instance. • Acclimatization begins in them in infancy. • The chest size is greatly increased. • Their hearts are considerably larger than those of lowlanders
ACUTE MOUNTAIN SICKNESS • This is also called as “High Altitude Pulmonary Edema.” • This occurs in a small number of lowlanders who ascend rapidly to high altitudes. • Begins from a few hours up to 2 days after their ascent. • Is serious and results in their death unless they are given Oxygen or taken to a low altitude.
ACUTE MOUNTAIN SICKNESS : SYMPTOMS & SIGNS • Acute Cerebral Edema: • Hypoxia causes cerebral vasodilatation • Increases capillary pressure • Causes fluid to leak out into the tissues • This leads to cerebral edema causing: • Severe disorientation • Other cerebral dysfunctions
ACUTE MOUNTAIN SICKNESS : SYMPTOMS & SIGNS • Acute Pulmonary Edema: • Severe hypoxia causes Pulmonary arteriolar constriction. • In some areas it is more and causes edema. • This can extend progressively to other areas of the lungs. • Can be reversed within hours on Oxygen therapy
CHRONIC MOUNTAIN SICKNESS • Seen in people who reside for long at high altitudes. • Red cell number and mass increases exceptionally. • Pulmonary arterial pressure becomes very high. • The heart becomes enlarged in the right side. • The peripheral arterial pressure begins to fall • Congestive Cardiac failure & death follows • They need to be taken to low altitudes as soon as possible. • They recover in low altitudes within days or weeks.
PHYSIOLOGICAL RESPONSES TO HIGH ALTITUDE HYPOXIA: • Arbitrarily Divided into following two--- • Acute responses (aka accommodation) • Long term responses ( aka acclimatization) • “Arbitrary” because ---- • Acute are also beneficial for long-term coping up. ii) Acute are modified steadily & imperceptibly in such a way that after 2-3 days are considered as beginninng of acclimatization . iii) Sharpness of division depends on rate of ascent .
ACCOMMODATION AT HIGH ALTITUDE: • immediate reflex responses of the body to acute hypoxic exposure. • Hyperventilation: arterial PO2 stimulation of peripheral chemoreceptors increased rate & depth of breathing B) Tachycardia: Also d/t peripheral chemo. Response CO oxygen delivery to the tissues
Contd….. • Increased 2,3-DPG conc. in RBC: within hours, ↑deoxy-Hb conc. locally ↑pH ↑2,3-DPG ↓oxygen affinity of Hb tissue O2 tension maintained at higher than normal level D) Neurological : • Considered as “warning signs” • Depression of CNS feels lazy, sleepy ,headache • ‘Release Phenomena’ like effect of alcohol • At further height cognitive impairment, twitching, convulsion & finally unconsciousness
ACCLIMATIZATION AT HIGH ALTITUDE: • Delivery of atmospheric O2 to the tissues normally involve 3 stages---with a drop in PO2 at each stage. • When the starting PO2 is lower than normal, body undergoes acclimatization so as to— • ↓ pressure drop during transfer • ↑ oxygen carrying capacity of blood • ↑ ability of tissues to utilize O2 • With longer stay at high altitude ,body is able to adjust by certain physiological adaptations..
A)Sustained Hyperventilation: • Prolonged hyperventilation CO2 wash-out respiratory alkalosis renal compensation alkaline urine normalization of pH of blood & CSF withdrawal of central chemo-mediated respiratory depression net result is ↑resting pulmonary ventilation (by ~5 folds to 60L/min),primarily d/t ↑ in TV (upto 50% of VC) • Such powerful ventilatory drive is also possible as- • ↑sensitivity of chemo- mechs to PO2 & PCO2 • Somewhat ↓ in work of breathing make easy & less tiring
B) Other Respiratory Changes: • ↑ TLC :esp in high-landers(natives for generations) evidenced by relatively enlarged (barrel-shaped) chest l/t ↑ventilatory capacity in relation to body mass. • ↑ Diffusing capacity of lungs: d/t hypoxic pulmonary vasoconstriction Pul. Hypertension ↑ no. of pulmonary capillaries →existence of this effect is still debatable!!!
C)↑Vascularity of the Tissues: More capillaries open up in tissues than at sea-level (normal ~25 % at rest—remaining as ‘reserve’). This combined with systemic vasodilatation(also a hypoxic response) more O2 delivery to tissues. D) Cellular level changes: ↑ intracellular mitochondrial density ↑ conc. of cellular oxidative enzymes ↑ synthesis of Mb( O2-storing pigment) →all aimed to improve O2 utilization.
Cheyne-Stokes Respirations: • Above 10,000 ft (3,000 m) most people experience a periodic breathing during sleep. The pattern begins with a few shallow breathsincreases to deep sighing respirations falls off rapidly. • Respirations may cease entirely for a few secs& then shallow breaths begin again. During period of breathing-arrest, person often becomes restless & may wake with a sudden feeling of suffocation. • Can disturb sleeping patterns exhausting the climber. Acetazolamide is helpful in relieving this. Not considered abnormal at high altitudes. But if occurs first during an illness (other than Altitude illnesses) or after an injury (particularly a head injury) may be a sign of a serious disorder.