Download
1 / 16
160 likes | 483 Views
Cardiac Electrophysiology, Perioperative Implications, Pacemakers/AICD. Todd Akins, MD April 28 th , 2009. Intraoperative ECG. No Contraindications

E N D
Cardiac Electrophysiology, Perioperative Implications, Pacemakers/AICD Todd Akins, MD April 28th, 2009
Intraoperative ECG • No Contraindications • ASA Standards “Every patient receiving anesthesia shall have the electrocardiogram continuously displayed from the beginning of anesthesia until preparing to leave the anesthetizing location.”
Detects • Dysrhythmias, myocardial ischemia, conduction abnormalities, pacemaker malfunction, and electrolyte disturbances
3-Lead vs 5-Lead • 3-Lead: lead II axis parallels atria thus greatest p-wave voltage (rate determination) • Provides enhanced diagnosis of arrhythmias and inferior wall ischemia
3-Lead vs 5-Lead • 5-Lead: only way to get a “true” V5 • Lead V5 placed at 5th ICS, anterior axillary line • Detects anterior and lateral wall ischemia • “Modified V5” with a 3-Lead by placing LA at the V5 position (5th ICS, AAL) and selecting lead I for display
Ideally • Lead II and Lead V5 monitored simultaneously with a 5-Lead • Use a 5-Lead in obese patients • If monitoring only a single lead, then choose lead to monitor based on patient’s history of prior ischemia or infarct (i.e. II if inferior MI, V5 if anterior or lateral)
Artifact • Caused by patient or lead wire movement, electrocautery, 60 cycle interference, faulty electrodes • Monitoring filters help but can distort ST segments • Monitor confuses large t-waves or artifact as QRS complexes • Better conductance by cleaning skin with alcohol or degreaser, or exfoliating area
Intraoperative MI • Commonly accepted criteria: • 1. flat or down sloping ST > 2mV, particularly with t-wave inversion • 2. ST segment elevation and peaked t-waves • *** Make sure volume is loud enough to hear while attention is elsewhere***
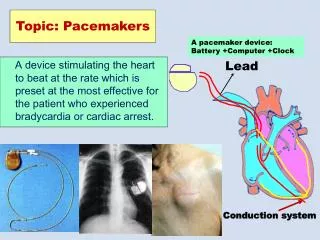
Pacemakers • Classification: • 5-letter code (usually omit last 2 letters) • Chamber Paced ( O, A, V, D) • Chamber Sensed (O, A, V, D) senses p or r • Response to Sensing (O, T, I, D) • Programmability (O, P, M, C, R) • Antitachyarrhythmia Function (O, P, S, D) • Most common: VVI, DDD, or on tests DVI
Functioning • If intrinsic HR < program (typically 72) then see spike then QRS and palpable pulse (100% capture) • If intrinsic HR > program, NO spike • When low battery, sensing lost before pacing output • Magnet defaults to VOO mode
Interference • Electrocautery Interferes • Interpreted as intrinsic function and can suppress pacemaker • Solution is to place grounding pad as far from pacemaker as possible • ***mandatory continuous monitoring of arterial pulse during cautery by palpation or pulse oximetry
PEARL • ***accentuated myospasticity from succinylcholine induced fasciculation or post-operative shivering can also suppress pacemaker
Operative Implications • NO MRI------EVER • ECT is fine, but have magnet available • ESWL: • 1. risk of developing arrhythmias • 2. shock waves can damage components • Contact manufacturer for best method of managing device, i.e. Reprogram vs. magnet • Time ESWL shock wave to 20msec after r-wave to decrease incidence of arrhythmias
AICD • Turn Off
References • 1. Morgan GE, Mikhail MS, Murray MJ, Clinical Anesthesiology, 3rd ed., New York, McGraw-Hill, 2002, pp. 97-100, 124-125, 431-432 • 2. Chu, LF, clinical Anesthesiology Board Review, A Test Simulation and Self-Assessment Tool, McGraw-Hill, 2005, pp. 231-232