Download

1 / 26
270 likes | 500 Views
醫學六 梁華昌 黃哲緯 王劭中. Discussion. Outline. Uterine cancer following breast cancer Risk: Breast cancer→ second primary cancer Risk: Tamoxifen → endometrial cancer Monitor: Tamoxifen → endometrial lesions Role of image: Diagnosis of endometrial abnormalities:

E N D
醫學六 梁華昌 黃哲緯 王劭中 Discussion
Outline Uterine cancer following breast cancer Risk: Breast cancer→ second primary cancer Risk: Tamoxifen → endometrial cancer Monitor: Tamoxifen → endometrial lesions Role of image: Diagnosis of endometrial abnormalities: Trans-vaginal ultrasound VS Hysteroscopy Adenosarcoma Adenosarcoma with sarcomatous overgrowth
Increased Risk for Second Primary Malignancies in Women with Breast Cancer Diagnosed at Young Age: A Population-Based Study in Taiwan Lee KD et al. Cancer Epidemiol Biomarkers Prev 2008;17(10) Population-based (n=53,783) Standardized incidence ratio
Nine second primary cancers had significant higher risk Bone, corpus uteri, ovary nonmelanoma skin, thyroid Esophagus, leukemia/lymphoma, kidney ,lung
Tamoxifen-Treatment for Breast Cancerand Risk of Endometrial cancer: a casecontrol study • Control: 1067 breast cancer patients with no subsequent endometrial cancer • Case:813 breast cancer patients who had subsequent endometrial cancer Swerdlow AJ, et al. JNCI J Natl Cancer Inst. 2005;97(5): 375-384
Tamoxifen use (yes vs no): cancer risk, OR =2.4 • Duration of treatment positively associated with endometrial cancer OR = 1.3 (< 2y ) increased to 7.2 (10-17y) Swerdlow AJ, et al. J Natl Cancer Inst. 2005 ;97(5):375-84.
Increasing daily dosage did not increase the risk of endometrial cancer Swerdlow AJ , et al. J Natl Cancer Inst. 2005;97(5):375-84.
Histology Type • Endometrial adenocarcinoma and mucinous carcinoma • OR = 2.1, p < 0.001 • Clear cell and papillary serous carcinoma • OR = 3.1, p = 0.119 • Mullerian and mesodermal mixed tumor and sarcoma • OR = 13.5, p<0.001 Swerdlow AJ, et al. J Natl Cancer Inst. 2005 ;97(5):375-84.
Treatment • No association with chemotherapy and non-tamoxifen hormonal therapy • Decreased risk with radiotherapy (RT) to breast area • OR = 0.7, p = 0.002 • Increased risk with RT to pelvic area • OR = 11.7, p = 0.012 Swerdlow AJ, et al. J Natl Cancer Inst. 2005 ;97(5):375-84.
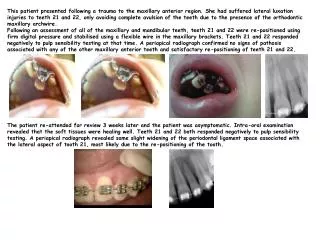
Diagnostic Approaches to Endometrial Lesions in Patients taking Tamoxifen
Role of Ultrasound and Hysteroscopy in Early Detection of Endometrial Abnormalities
Transvaginal Ultrasound (TV-US) • Review of 35 studies, 5892 women, for detecting endometrial abnormalities • Sensitivity 92~96%; specificity 61~80% Smith-Bindman R, et al. JAMA. 1998;280(17):1510-7. • 53 breast cancer women treated with tamoxifen • Sensitivity 92%; specificity 80% Timmerman D, et al. Am J Obstet Gynecol. 1998;179(1):62-70. • 247 tamoxifen-treated women and 98 controls • High false-positive rate 46% Gerber B, et al. J Clin Oncol. 2000;18(20):3464-70. Love CD, et al . J Clin Oncol. 1999;17(7):2050-4.
Hysteroscopy • Quantitative systematic review of 65 studies, including 26,346 women • Highly accurate in diagnosing endometrial cancer • Sensitivity 86.4%; Specificity 99.2% Clark TJ,et al. JAMA. 2002;288(13):1610-21. • Retrospective study of patients with endometrial cancer underwent hysteroscopy (69) or not (112) • Sensitivity 93.10%; specificity 99.96% Marchetti M, et al. Eur J Gynaecol Oncol. 2002;23(2):151-3.
Ultrasound vs Hysteroscopy • 5 systemic review studies • Transvaginal ultrasound • excluding endometrial cancer in women with abnormal vaginal bleeding • Hysteroscopy • Effectively detecting endometrial cancer, but less effective at excluding seriousat excluding seriousdisease Clark TJ, et al. Curr Opin Obstet Gynecol. 2004;16(4):305-11. • TV-US was cost-effective in initial evaluating abnormal bleeding Clark TJ, et al.BJOG. 2006;113(5):502-10.
Adenosarcoma • Prevalence • Uterine sarcomas account for approximately1% of female genital tract malignancies and 3-7% of uterine cancers Major FJ, et al. Cancer. 1993;71:1702–9. • Adenosarcomas account for 5.5% of uterine sarcomas Abeler VM, et al. Histopathology. 2009;54:355–364.
MullerianAdenosarcoma With Sarcomatous Overgrowth (MASO) • First introduced by Clement and Scully in 1989 • More than 25% of the adenosarcoma is composed of pure sarcoma Clement PB, et al. Am J Surg Pathol. 1989;13:28–38. • Uterine MASO: • an aggressive variant of adenosarcoma • overall survival was similar with that of malignant mixed müllerian tumors Krivac T, et al. Gynecol Oncol. 2001; 83: 89–94.
Recurrence • Occurs in 38% of cases (n=41) • Median time to recurrence is 12 months Verschraegen CF, et al. Oncol Rep. 1998;5(4):939-44. • Recurrences are mostly composed of solely sarcoma which is always higher grade than the original tumor Clement PB, et al. Cancer. 1974;34(4):1138-49.
Predictors of Recurrence • Clinical: • Extrauterine spread and myometrial invasion were associated with higher rates of recurrence Clement PB, et al. Cancer. 1974;34(4):1138-49 Kaku T, et al. Int J Gynecol Pathol. 1992;11(2):75-88 • Pathological: • 44%in sarcomatous overgrowth compared to 14% in adenosarcomas without sarcomatous overgrowth Kaku T, et al. Int J Gynecol Pathol. 1992;11(2):75-88
Treatment • Hysterectomy with bilateral salpingo-oophorectomy Amant F, et al. Lancet Oncol. 2009 ;10(12):1188-98 • Adjuvant radiotherapy appears to have a role in better pelvic control and decrease in local recurrence of the tumor. • Chemotherapy: doxorubicin, ifosfamide, and cisplatin. Acharya S, et al. Lancet Oncol. 2005;6(12):961-71
Mullerian Adenosarcoma with Sarcomatous Overgrowth Review of Case Reports
Search in Pubmed Key word: uterine adenosarcoma Total 14 papers, including 54 patients were reported adenosarcoma with sarcomatous overgrowth Clinical data were only found in 14 patients
Age • Range from 33 to 80 years (mean: 55.6 years) • Treatment • Alltreated with (TAH+BSO), with or without radiotherapy and chemotherapy • Stage • 4/14 (29%) patients was diagnosed as stage IV dx at diagnosis
Recurrence • 10 out of 14 (71.4%) • Site: pelvis, abdomen, lung • Survival • 7/14 (50%) patients died within 2 months after diagnosis • Within these 7 expired patients, only 2 patients didn’t receive adjuvant therapy