Download
1 / 63
740 likes | 1.32k Views
Spinal Cord Infarction. Stroke Rounds January 12, 2011 Sandra Derghazarian. Case Presentation: Mr. B. Background Information. Called Friday at 11am for “R/o cauda equina”. 69M POD#2 PMHx: Lung adenocarcinoma DM II x 15 yrs CRF PVD s/p fem-fem bypass Ischemic CMP HTN, DLP

E N D
Spinal Cord Infarction Stroke Rounds January 12, 2011 Sandra Derghazarian
Background Information • Called Friday at 11am for “R/o cauda equina” • 69M POD#2 • PMHx: • Lung adenocarcinoma • DM II x 15 yrs • CRF • PVD s/p fem-fem bypass • Ischemic CMP • HTN, DLP • Hypothyroidism • Ex-smoker (55 pk-yr) • Meds • ASA and Plavix - held • Telmisartan, hydralazine • Simvastatin • Furosemide, metolazone • Synthroid • Insulin • Epidural,T4-T5 level • Bupivacaine, fentanyl
HPI • Admitted for lobectomy on November 23 • Surgery on November 24 • Thoracotomy with RM+RU lobectomies • Systolic BP 80 x 5 min, 90 x 60 min • Early post-op course • Acute on chronic kidney failure • Planned for PET scan on POD#2 • Insulin infusion stopped prior evening
HPI • 6-7 am of POD#2 • Ambulated to bathroom with some assistance • 8:30 am • Found unresponsive in chair • BP initially unmeasurable, glucose > 30 • BP 96/40, HR 93 • Resuscitated with fluids, insulin • sBP 125mmHg, glucose 10
HPI • LOC improved • C/o lower extremity numbness • Noted to have lower extremity weakness • Anesthesia called • Epidural infusion stopped and given naloxone • One hour later, persistent numbness and weakness • We were called...
On Exam • VS 126/49, HR 56, RR 20, O2 98% R/A • Mental status • Oriented to time, place, situation • Cranial nerves • Pupils bilat round, reactive; EOM and VF intact • Normal sensation, no asymmetry • Normal palate elevation, tongue midline
On Exam • Motor exam • Decreased tone in lower extremities • Power • No rectal tone
On Exam • Reflexes • Absent DTRs bilaterally, upper/lower extremities • Toes mute • Sensory • T4 level for pinprick and temperature • Vibration sensation absent at toes, ankles • JPS and light touch intact in lower and upper extremities
Investigations • CBC and coags • Hg 95 (baseline 110) • WBC 11.60 (9.60) • Plt 142 • INR 1.17 • Electrolytes/Renal function • K+ 5.9, Cr 314 (baseline 150) • Troponin 0.88 1.17 • EKG – ventricular bigeminy • Bone scan - Negative for mets October 2010
Next Step • Spinal cord infarct • R/o epidural hematoma • R/o compression from lung mets • T-L-S spine MRI • Performed 6 hours after onset of symptoms
MRI • No compressive pathologies • Imaging and clinical findings consistent with diagnosis of spinal cord infarct • Most likely secondary to hypotensive episode in a vasculopathic pt • Re-initiate antiplatelet therapy as soon as possible • Maintain adequate BP
In-Hospital Course • 3 days later, pt noted to have atrial fibrillation • Started on anticoagulation • TEE – r/o cardioembolic source of SCI • Severe biatrial enlargement • No clot or smoke in LV or LAA • No evidence endocarditis • No previously documented afib
In-Hospital Course • Requires assist x 2 for ambulation • T4 sensory level PP/Temp • Bowel/Bladder symptoms • Urinary retention • Fecal incontinence • Other complications • Lower GI bleed secondary to rectal ulcers • Pressure sores
Outline • Vascular anatomy • Neurovascular syndromes • Etiologies • Diagnosis & Imaging • Management & Outcomes
“All our words are but crumbs that fall from the feast of our mind” - Kahlil Gibran
Vascular Anatomy “Despite the clinical importance of the spinal cord blood supply, the extensive literature on this subject is both confusing and inconsistent.”
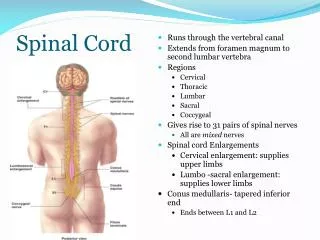
Vascular Anatomy • Supply via extrinsic and intrinsic arteries • Extrinsic • Anterior and posterior longitudinal spinal arteries • Radiculomedullary arteries • Pial plexus • Intrinsic • Central or sulcal branches of ASA • Perforating branches of PSA and pial plexus
Longitudinal Spinal Arteries • Originate from VA • Anterior: single • Posterior: paired • Course longitudinally along spinal cord • Provide blood supply to the spinal cord via intrinsic branches • Central or sulcal branches • Perforating branches • Supplied at intervals by radiculomedullary arteries
Origin of Radicular Arteries • Segmental/intercostal artery, post branch • Spinal artery (intervert. foramen) • Ant and post canal arts (vert., dura, ligaments) • Radicular artery (nerve roots, ant and post) • Radiculomedullary arteries • Anterior and posterior branches • Supply ASA and PSA • Variable number • 5-8 anteriorly, 10-20 posteriorly
Radicular Arteries • Divided into groups based on origin and area supplied: • Cervicothoracic (C1-T3) • C3 level , from VA • C6-7, from cervical ascending arteries • Middle thoracic (T3 to T8) • Usually from single T7 radicular artery • Thoracolumbar (T8 to cone) • From large T8 – L1 anterior radicular artery or artery of Adamkiewicz • +/- cone artery originating from the internal iliac artery
Intrinsic vessels Penetrating branches Sulcal artery
Clinical Neurovascular Syndromes • Understanding of vascular anatomy has led to recognition of well-known spinal stroke syndromes • Anterior spinal artery syndrome • Most common • Interruption of ASA or radicular artery • Infarction of anterior 2/3 of cord • Abrupt onset flaccid paraplegia, areflexia, loss of spinothalamic perception, autonomic deficits
Clinical Neurovascular Syndromes • Brown-Séquard syndrome • Interruption of sulcal artery • Ipsilateral paralysis and contralateral loss of spinothalamic sensation • Posterior spinal artery syndrome • Interruption of PSA • Infarction of posterior 1/3 • Impaired proprioception and vibration sense • May also develop weakness
Epidemiology • Account for about 1% of all strokes • Incidence has not been specifically reported • Estimate of 5,000 – 8,000 cases in US per year
Etiology • Diverse spectrum of processes can lead to interruption of vascular supply • Etiologic subgroups • Aortic disease • Systemic hypoperfusion • Cardiogenic embolism • Vasculitis • Infection • Non-aortic surgery • Spine disease
Etiology • Case series of SCI • 44 patients, aged 15 – 90 Neurology 1996;47:321
Etiology • Other reported etiologies • Vertebral artery dissection • Fibrocartilagenous embolism • Disc herniation • Cocaine use • Surfing • Depending on series, 7-35% cryptogenic
Diagnosis • Suspect on basis of clinical manifestation • Pattern of deficit consistent with spinal neurovascular syndrome • Abrupt onset (minutes to hours) • Presence of neck or back pain in 60-70% • May have radicular pain at level of lesion • Imaging is key • R/o compressive myelopathy
Diagnosis • MRI abnormalities on T2-WI • Present as early as 4 hours of symptom onset • In case series, 45-72% of lesions visualised • Sagittal view • Central “pencil-like” hyperintensity • Cord enlargement • Axial view • Symmetric or asymmetric hyperintensities
Diagnosis • What about DWI? • Case series looking at use of DWI in acute SCI • DWI helpful for confirmation • Unknown sensitivity and specificity for ischemic lesions • Do not yet know false positives/negatives • Consider clinical context • Combine with T2 for better resolution
Diagnosis • Further investigations depend on clinical context • R/o aortic dissection with CT or MRI • R/o VA dissection with CTA/MRA if C-spine infarct • R/o cardioembolic source with TTE/TEE • R/o infectious or inflammatory causes • CSF (cell count, protein, OCB, Lyme, syphilis) • Serum (ANA, ANCA, VDRL, Lyme, HIV, CMV, HSV, VZV)
Management • Non-surgical SCI • No specific treatments have been investigated • SCI due to aneurysm repair • Specific interventions for SCI • Blood pressure optimisation • CSF drain
Management – Case series • de Seze et al. Brain 2001;124:1509-1520 • Retrospective study of acute myelopathy cases • 11 cases of SCI (79 total) • 4 treated with corticosteroids • 7 anticoagulated with heparin • ASA for 2ary prevention in all • Outcomes • No clear efficacy of either treatment • Recovery poor to fair in 91% • Require assistance to walk >100m, sphincter dysfctn